10.Adrenoceptor Antagonist Drugs Brian B.Hoffmnan,MD INTRODUCTION Since catecholamines play a role in a variety of physiologic and pathophysiologic responses,drugs that block adrenoceptors have important effects,some of which are of great clinical value.These effects vary dramatically according to the drug's selectivity for a and b receptors.The classification of adrenoceptors into a,a2,and b subtypes and the effects of activating these receptors are discussed in Chapters 6 and 9.Blockade of peripheral dopamine receptors is of no recognized clinical importance at present.In contrast,blockade of central nervous system dopamine receptors is very important;drugs that act on these receptors are discussed in Chapters 21 and 29.This chapter deals with pharmacologic antagonist drugs whose major effect is to occupy either ai,az,or b receptors outside the central nervous system and prevent their activation by catecholamines and related agonists. For pharmacologic research,ai-and az-adrenoceptor antagonist drugs have been very useful in the experimental exploration of autonomic nervous system function.In clinical therapeutics,nonselective a antagonists are used in the treatment of pheochromocytoma(tumors that secrete catecholamines),and ai-selective antagonists are used in primary hypertension and benign prostatic hyperplasia.Beta-receptor antagonist drugs have been found useful in a much wider variety of clinical conditions and are firmly established in the treatment of hypertension,ischemic heart disease, arrhythmias,endocrinologic and neurologic disorders,glaucoma,and other conditions. I.BASIC PHARMACOLOGY OF THE ALPHA-RECEPTOR ANTAGONIST DRUGS Mechanism of Action Alpha-receptor antagonists may be reversible or irreversible in their interaction with these receptors.Reversible antagonists dissociate from receptors and the block can be surmounted with sufficiently high concentrations of agonists;irreversible drugs do not dissociate and cannot be surmounted.Phentolamine(Figure 10-1)and prazosin are examples of reversible antagonists.Prazosin (and analogs)and labetaloldrugs used primarily for their antihypertensive effects%as well as several ergot derivatives(see Chapter 16)are also reversible a-adrenoceptor antagonists or partial agonists. Phenoxybenzamine,an agent related to the nitrogen mustards,forms a reactive ethyleneimonium intermediate(Figure 10-1)that covalently binds to a receptors, resulting in irreversible blockade.Figure 10-2 illustrates the effects of a reversible drug in comparison with those of an irreversible agent
10. Adrenoceptor Antagonist Drugs ¾ Brian B. Hof man, MD INTRODUCTION Since catecholamines play a role in a variety of physiologic and pathophysiologic responses, drugs that block adrenoceptors have important effects, some of which are of great clinical value. These effects vary dramatically according to the drug's selectivity for a and b receptors. The classification of adrenoceptors into a1, a2, and b subtypes and the effects of activating these receptors are discussed in Chapters 6 and 9. Blockade of peripheral dopamine receptors is of no recognized clinical importance at present. In contrast, blockade of central nervous system dopamine receptors is very important; drugs that act on these receptors are discussed in Chapters 21 and 29. This chapter deals with pharmacologic antagonist drugs whose major effect is to occupy either a1, a2, or b receptors outside the central nervous system and prevent their activation by catecholamines and related agonists. For pharmacologic research, a1- and a2-adrenoceptor antagonist drugs have been very useful in the experimental exploration of autonomic nervous system function. In clinical therapeutics, nonselective a antagonists are used in the treatment of pheochromocytoma (tumors that secrete catecholamines), and a1-selective antagonists are used in primary hypertension and benign prostatic hyperplasia. Beta-receptor antagonist drugs have been found useful in a much wider variety of clinical conditions and are firmly established in the treatment of hypertension, ischemic heart disease, arrhythmias, endocrinologic and neurologic disorders, glaucoma, and other conditions. I. BASIC PHARMACOLOGY OF THE ALPHA-RECEPTOR ANTAGONIST DRUGS Mechanism of Action Alpha-receptor antagonists may be reversible or irreversible in their interaction with these receptors. Reversible antagonists dissociate from receptors and the block can be surmounted with sufficiently high concentrations of agonists; irreversible drugs do not dissociate and cannot be surmounted. Phentolamine (Figure 10-1) and prazosin are examples of reversible antagonists. Prazosin (and analogs) and labetalol¾drugs used primarily for their antihypertensive effects¾as well as several ergot derivatives (see Chapter 16) are also reversible a-adrenoceptor antagonists or partial agonists. Phenoxybenzamine, an agent related to the nitrogen mustards, forms a reactive ethyleneimonium intermediate (Figure 10-1) that covalently binds to a receptors, resulting in irreversible blockade. Figure 10-2 illustrates the effects of a reversible drug in comparison with those of an irreversible agent
As discussed in Chapters 1 and 2,the duration of action of a reversible antagonist is largely dependent on the half-life of the drug in the body and the rate at which it dissociates from its receptor:The shorter the half-life of the drug in the body,the less time it takes for the effects of the drug to dissipate.In contrast,the effects of an irreversible antagonist may persist long after the drug has been cleared from the plasma.In the case of phenoxybenzamine,the restoration of tissue responsiveness after extensive a-receptor blockade is dependent on synthesis of new receptors,which may take several days.The rate of return of a-adrenoceptor responsiveness may be particularly important in patients having a sudden cardiovascular event or who become candidates for urgent surgery. HO CH3 0-CH2-CH CH一CH一C CH N R2 CH2 Phentolamine Phenoxybenzamine Active(ethyleneimonium) intermediato CH30 Prazosin 0- CH2一CH2一NH一CH一CH SO-NH2 0- CH2一CH3 0一CH Tamsulosin 100 100 Control Control 50 50 10μmolL 0.4 umol/L 0.8 umol/L 20 umoVL 0 2.4 20 160 12 10 80 Norepinephrine(umol/L) Norepinephrine (umol/L)
As discussed in Chapters 1 and 2, the duration of action of a reversible antagonist is largely dependent on the half-life of the drug in the body and the rate at which it dissociates from its receptor: The shorter the half-life of the drug in the body, the less time it takes for the effects of the drug to dissipate. In contrast, the effects of an irreversible antagonist may persist long after the drug has been cleared from the plasma. In the case of phenoxybenzamine, the restoration of tissue responsiveness after extensive a-receptor blockade is dependent on synthesis of new receptors, which may take several days. The rate of return of a1-adrenoceptor responsiveness may be particularly important in patients having a sudden cardiovascular event or who become candidates for urgent surgery
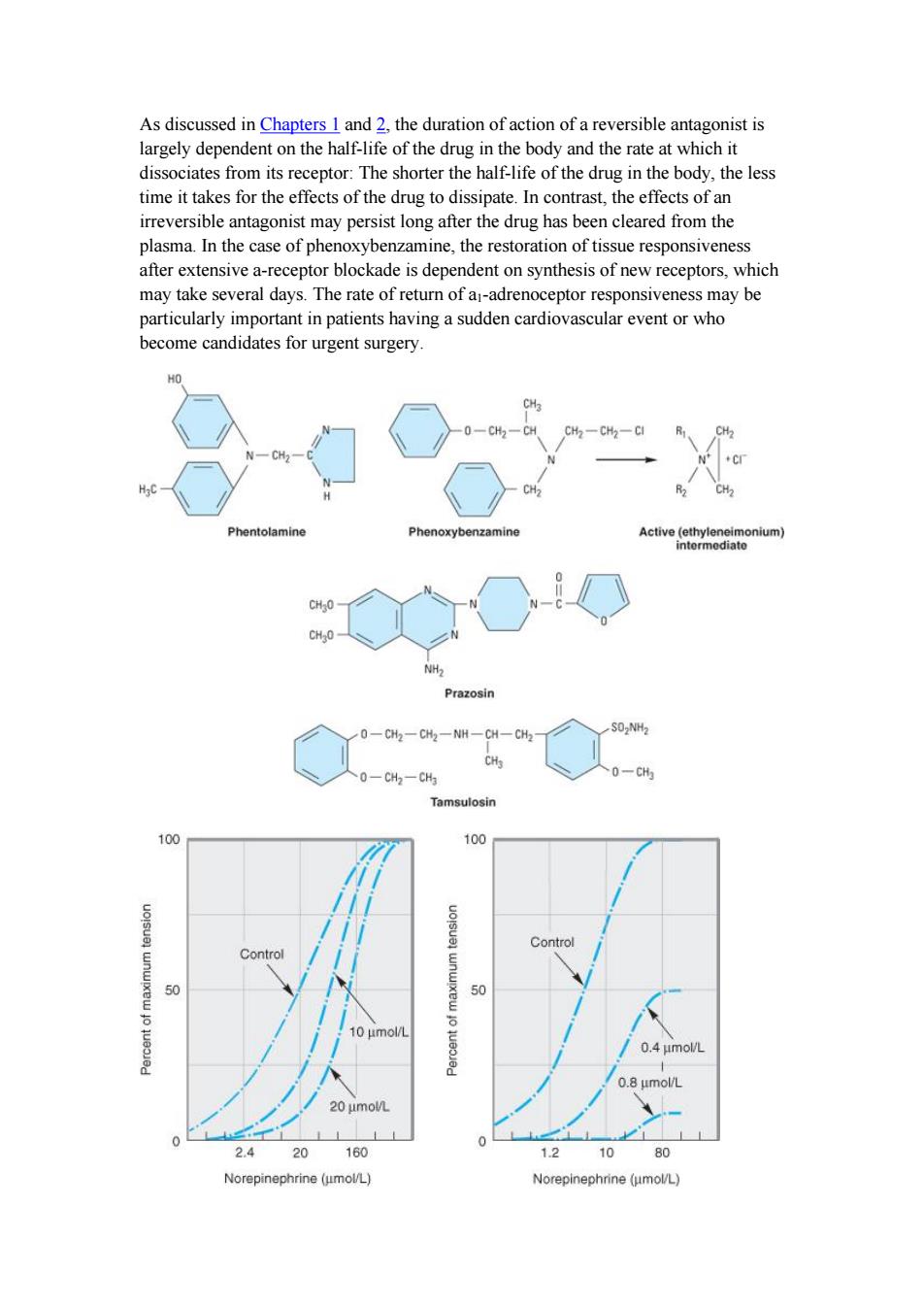
Figure 10-1.Structure of several a-receptor-blocking drugs. Figure 10-2.Dose-response curves to norepinephrine in the presence of two different a-adrenoceptor-blocking drugs.The tension produced in isolated strips of cat spleen, a tissue rich in a receptors,was measured in response to graded doses of norepinephrine.Left:Tolazoline,a reversible blocker,shifted the curve to the right without decreasing the maximum response when present at concentrations of 10 and 20 umol/L.Right:Dibenamine,an analog of phenoxybenzamine and irreversible in its action,reduced the maximum response attainable at both concentrations tested. (Modified and reproduced,with permission,from Bickerton RK:The response of isolated strips of cat spleen to sympathomimetic drugs and their antagonists.J Pharmacol Exp Ther 1963;142:99.) Pharmacologic Effects A.CARDIOVASCULAR EFFECTS Because arteriolar and venous tone are determined to a large extent by a receptors on vascular smooth muscle,a-receptor antagonist drugs cause a lowering of peripheral vascular resistance and blood pressure(Figure 10-3).These drugs can prevent the pressor effects of usual doses of a agonists;indeed,in the case of agonists with both a and b2 effects(eg,epinephrine),selective a-receptor antagonism may convert a pressor to a depressor response(Figure 10-3).This change in response is called epinephrine reversal;it illustrates how the activation of both a and b receptors in the vasculature may lead to opposite responses.Alpha-receptor antagonists often cause postural hypotension and reflex tachycardia;nonselective(ai=a2,Table 10-1) blockers usually cause significant tachycardia if blood pressure is lowered below normal.Postural hypotension is due to antagonism of sympathetic nervous system stimulation of ai receptors in venous smooth muscle;contraction of veins is an important component of the normal capacity to maintain blood pressure in the upright position since it decreases venous pooling in the periphery.Constriction of arterioles in the legs may also contribute to the postural response.Tachycardia may be more marked with agents that block a2-presynaptic receptors in the heart,since the augmented release of norepinephrine will further stimulate b receptors in the heart. B.OTHER EFFECTS Minor effects that signal the blockade of a receptors in other tissues include miosis and nasal stuffiness.Alphai-receptor blockade of the base of the bladder and the prostate is associated with decreased resistance to the flow of urine.Individual agents may have other important effects in addition to a-receptor antagonism(see below)
Figure 10-1. Structure of several a-receptor-blocking drugs. Figure 10-2. Dose-response curves to norepinephrine in the presence of two different a-adrenoceptor-blocking drugs. The tension produced in isolated strips of cat spleen, a tissue rich in a receptors, was measured in response to graded doses of norepinephrine. Left: Tolazoline, a reversible blocker, shifted the curve to the right without decreasing the maximum response when present at concentrations of 10 and 20 umol/L. Right: Dibenamine, an analog of phenoxybenzamine and irreversible in its action, reduced the maximum response attainable at both concentrations tested. (Modified and reproduced, with permission, from Bickerton RK: The response of isolated strips of cat spleen to sympathomimetic drugs and their antagonists. J Pharmacol Exp Ther 1963;142:99.) Pharmacologic Effects A. CARDIOVASCULAR EFFECTS Because arteriolar and venous tone are determined to a large extent by a receptors on vascular smooth muscle, a-receptor antagonist drugs cause a lowering of peripheral vascular resistance and blood pressure (Figure 10-3). These drugs can prevent the pressor effects of usual doses of a agonists; indeed, in the case of agonists with both a and b2 effects (eg, epinephrine), selective a-receptor antagonism may convert a pressor to a depressor response (Figure 10-3). This change in response is called epinephrine reversal; it illustrates how the activation of both a and b receptors in the vasculature may lead to opposite responses. Alpha-receptor antagonists often cause postural hypotension and reflex tachycardia; nonselective (a1 = a2, Table 10-1) blockers usually cause significant tachycardia if blood pressure is lowered below normal. Postural hypotension is due to antagonism of sympathetic nervous system stimulation of a1 receptors in venous smooth muscle; contraction of veins is an important component of the normal capacity to maintain blood pressure in the upright position since it decreases venous pooling in the periphery. Constriction of arterioles in the legs may also contribute to the postural response. Tachycardia may be more marked with agents that block a2-presynaptic receptors in the heart, since the augmented release of norepinephrine will further stimulate b receptors in the heart. B. OTHER EFFECTS Minor effects that signal the blockade of a receptors in other tissues include miosis and nasal stuffiness. Alpha1-receptor blockade of the base of the bladder and the prostate is associated with decreased resistance to the flow of urine. Individual agents may have other important effects in addition to a-receptor antagonism (see below)
135/85 128/50 HR 160 200 Phentolamine 190/124 16082 175/110 135/90 HR 180 210 Epinephrine before phentolamine 125/85 100/35 HR 190 210 Epinephrine after phentolamine Figure 10-3.Top:Effects of phentolamine,an a-receptor-blocking drug,on blood pressure in an anesthetized dog.Epinephrine reversal is demonstrated by tracings showing the response to epinephrine before(middle)and after(bottom) phentolamine.All drugs given intravenously.(BP,blood pressure;HR,heart rate.) SPECIFIC AGENTS Phentolamine,an imidazoline derivative,is a potent competitive antagonist at both ar and az receptors(Table 10-1).Phentolamine causes a reduction in peripheral resistance through blockade of ai receptors and possibly az receptors on vascular smooth muscle.The cardiac stimulation induced by phentolamine is due to sympathetic stimulation of the heart resulting from baroreflex mechanisms. Furthermore,since phentolamine potently blocks az receptors,antagonism of presynaptic az receptors may lead to enhanced release of norepinephrine from sympathetic nerves.In addition to being an ai-and az-receptor antagonist, phentolamine also has minor inhibitory effects at serotonin receptors and agonist effects at muscarinic and Hi and H2 histamine receptors. Phentolamine has limited absorption after oral administration.Its pharmacokinetic properties are not well known;it may reach peak concentrations within an hour after oral administration and has a half-life of 5-7 hours.The principal adverse effects are related to cardiac stimulation,which may cause severe tachycardia,arrhythmias,and myocardial ischemia,especially after intravenous administration.With oral administration,adverse effects include tachycardia,nasal congestion,and headache
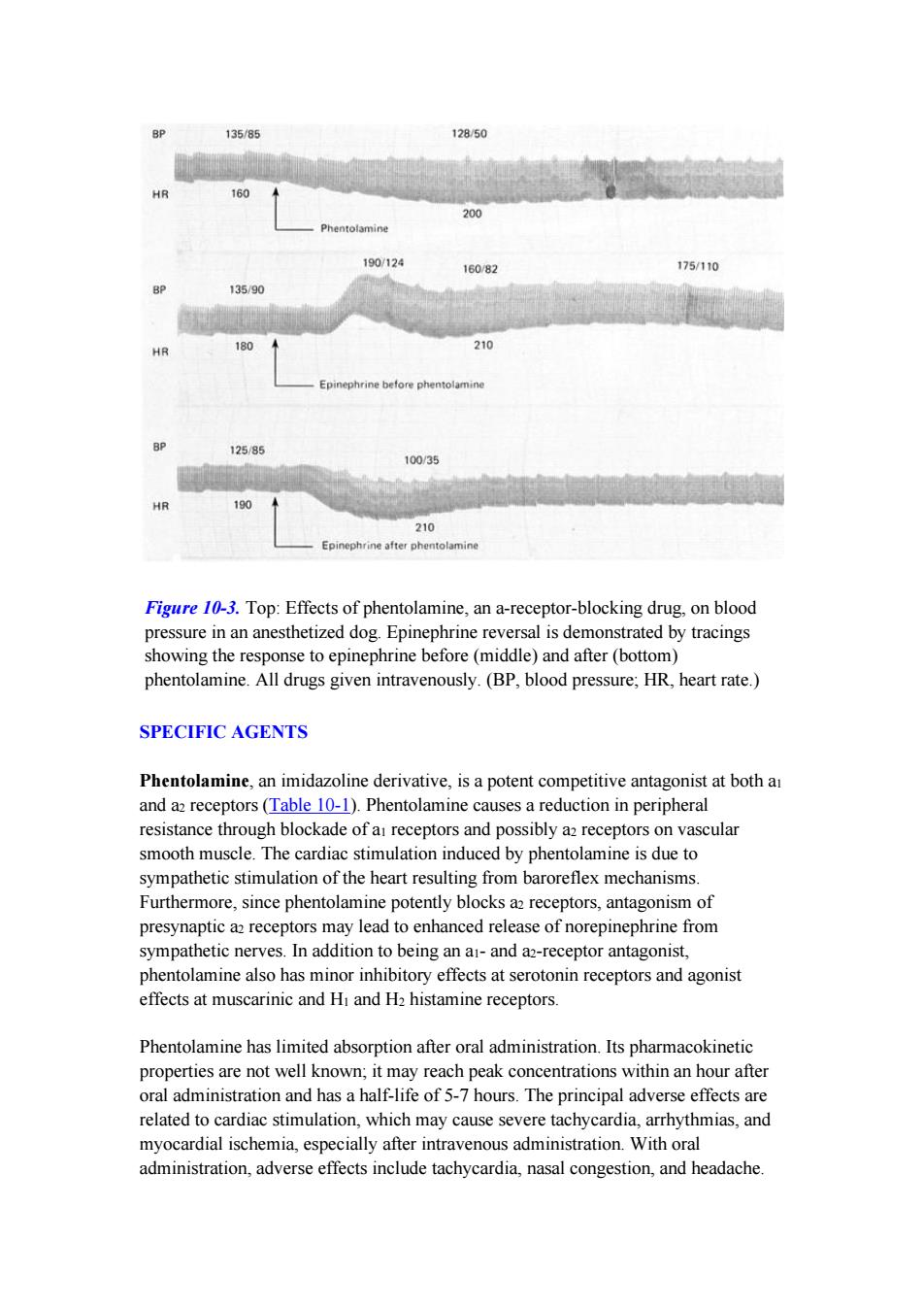
Figure 10-3. Top: Effects of phentolamine, an a-receptor-blocking drug, on blood pressure in an anesthetized dog. Epinephrine reversal is demonstrated by tracings showing the response to epinephrine before (middle) and after (bottom) phentolamine. All drugs given intravenously. (BP, blood pressure; HR, heart rate.) SPECIFIC AGENTS Phentolamine, an imidazoline derivative, is a potent competitive antagonist at both a1 and a2 receptors (Table 10-1). Phentolamine causes a reduction in peripheral resistance through blockade of a1 receptors and possibly a2 receptors on vascular smooth muscle. The cardiac stimulation induced by phentolamine is due to sympathetic stimulation of the heart resulting from baroreflex mechanisms. Furthermore, since phentolamine potently blocks a2 receptors, antagonism of presynaptic a2 receptors may lead to enhanced release of norepinephrine from sympathetic nerves. In addition to being an a1- and a2-receptor antagonist, phentolamine also has minor inhibitory effects at serotonin receptors and agonist effects at muscarinic and H1 and H2 histamine receptors. Phentolamine has limited absorption after oral administration. Its pharmacokinetic properties are not well known; it may reach peak concentrations within an hour after oral administration and has a half-life of 5-7 hours. The principal adverse effects are related to cardiac stimulation, which may cause severe tachycardia, arrhythmias, and myocardial ischemia, especially after intravenous administration. With oral administration, adverse effects include tachycardia, nasal congestion, and headache
Phentolamine has been used in the treatment of pheochromocytomaespecially intraoperativelyas well as for male erectile dysfunction by injection intracavernosally and when taken orally (see below). Phenoxybenzamine binds covalently to a receptors,causing irreversible blockade of long duration(14-48 hours or longer).It is somewhat selective for a receptors but less so than prazosin(Table 10-1).The drug also inhibits reuptake of released norepinephrine by presynaptic adrenergic nerve terminals.Phenoxybenzamine blocks histamine (Hi),acetylcholine,and serotonin receptors as well as a receptors (see Chapter 16) The pharmacologic actions of phenoxybenzamine are primarily related to antagonism of a-receptor-mediated events.Most significant is that phenoxybenzamine attenuates catecholamine-induced vasoconstriction.While phenoxybenzamine causes relatively little fall in blood pressure in normal supine individuals,it reduces blood pressure when sympathetic tone is high,eg,as a result of upright posture or because of reduced blood volume.Cardiac output may be increased because of reflex effects and because of some blockade of presynaptic az receptors in cardiac sympathetic nerves. Phenoxybenzamine is absorbed after oral administration,although bioavailability is low and its kinetic properties are not well known.The drug is usually given orally, starting with low doses of 10-20 mg/d and progressively increasing the dose until the desired effect is achieved.A dosage of less than 100 mg/d is usually sufficient to achieve adequate a-receptor blockade.The major use of phenoxybenzamine is in the treatment of pheochromocytoma(see below). Many of the adverse effects of phenoxybenzamine derive from its a-receptor-blocking action;the most important are postural hypotension and tachycardia.Nasal stuffiness and inhibition of ejaculation also occur.Since phenoxybenzamine enters the central nervous system,it may cause less specific effects,including fatigue,sedation,and nausea.Because phenoxybenzamine is an alkylating agent,it may have other adverse effects that have not yet been characterized.Phenoxybenzamine causes tumors in animals,but the clinical implications of this observation are unknown. Tolazoline is an obsolete agent similar to phentolamine.Ergot derivatives,eg, ergotamine,dihydroergotamine,cause reversible a-receptor blockade,probably via a partial agonist action (Chapter 16). Prazosin is a piperazinyl quinazoline effective in the management of hypertension (see Chapter 11).It is highly selective for ai receptors and typically 1000-fold less potent at az receptors.This may partially explain the relative absence of tachycardia seen with prazosin compared with that reported with phentolamine and phenoxybenzamine.Prazosin leads to relaxation of both arterial and venous vascular
Phentolamine has been used in the treatment of pheochromocytoma¾especially intraoperatively¾as well as for male erectile dysfunction by injection intracavernosally and when taken orally (see below). Phenoxybenzamine binds covalently to a receptors, causing irreversible blockade of long duration (14-48 hours or longer). It is somewhat selective for a1 receptors but less so than prazosin (Table 10-1). The drug also inhibits reuptake of released norepinephrine by presynaptic adrenergic nerve terminals. Phenoxybenzamine blocks histamine (H1), acetylcholine, and serotonin receptors as well as a receptors (see Chapter 16). The pharmacologic actions of phenoxybenzamine are primarily related to antagonism of a-receptor-mediated events. Most significant is that phenoxybenzamine attenuates catecholamine-induced vasoconstriction. While phenoxybenzamine causes relatively little fall in blood pressure in normal supine individuals, it reduces blood pressure when sympathetic tone is high, eg, as a result of upright posture or because of reduced blood volume. Cardiac output may be increased because of reflex effects and because of some blockade of presynaptic a2 receptors in cardiac sympathetic nerves. Phenoxybenzamine is absorbed after oral administration, although bioavailability is low and its kinetic properties are not well known. The drug is usually given orally, starting with low doses of 10-20 mg/d and progressively increasing the dose until the desired effect is achieved. A dosage of less than 100 mg/d is usually sufficient to achieve adequate a-receptor blockade. The major use of phenoxybenzamine is in the treatment of pheochromocytoma (see below). Many of the adverse effects of phenoxybenzamine derive from its a-receptor-blocking action; the most important are postural hypotension and tachycardia. Nasal stuffiness and inhibition of ejaculation also occur. Since phenoxybenzamine enters the central nervous system, it may cause less specific effects, including fatigue, sedation, and nausea. Because phenoxybenzamine is an alkylating agent, it may have other adverse effects that have not yet been characterized. Phenoxybenzamine causes tumors in animals, but the clinical implications of this observation are unknown. Tolazoline is an obsolete agent similar to phentolamine. Ergot derivatives, eg, ergotamine, dihydroergotamine, cause reversible a-receptor blockade, probably via a partial agonist action (Chapter 16). Prazosin is a piperazinyl quinazoline effective in the management of hypertension (see Chapter 11). It is highly selective for a1 receptors and typically 1000-fold less potent at a2 receptors. This may partially explain the relative absence of tachycardia seen with prazosin compared with that reported with phentolamine and phenoxybenzamine. Prazosin leads to relaxation of both arterial and venous vascular