
Pharmacologic Management of Parkinsonism Other Movement Disorders Michael J.Aminoff,MD,DSc,FRCP INTRODUCTION Several types of abnormal movement are recognized.Tremor consists of a rhythmic oscillatory movement around a joint and is best characterized by its relation to activity. Tremor at rest is characteristic of parkinsonism,when it is often associated with rigidity and an impairment of voluntary activity.Tremor may occur during maintenance of sustained posture(postural tremor)or during movement(intention tremor).A conspicuous postural tremor is the cardinal feature of benign essential or familial tremor.Intention tremor occurs in patients with a lesion of the brainstem or cerebellum,especially when the superior cerebellar peduncle is involved,and may also occur as a manifestation of toxicity from alcohol or certain other drugs. Chorea consists of irregular,unpredictable,involuntary muscle jerks that occur in different parts of the body and impair voluntary activity.In some instances,the proximal muscles of the limbs are most severely affected,and because the abnormal movements are then particularly violent,the term ballismus has been used to describe them.Chorea may be hereditary or may occur as a complication of a number of general medical disorders and of therapy with certain drugs. Abnormal movements may be slow and writhing in character(athetosis)and in some instances are so sustained that they are more properly regarded as abnormal postures (dystonia).Athetosis or dystonia may occur with perinatal brain damage,with focal or generalized cerebral lesions,as an acute complication of certain drugs,as an accompaniment of diverse neurologic disorders,or as an isolated inherited phenomenon of uncertain cause known as idiopathic torsion dystonia or dystonia musculorum deformans.Its physiologic basis is uncertain,and treatment is unsatisfactory. Tics are sudden coordinated abnormal movements that tend to occur repetitively, particularly about the face and head,especially in children,and can be suppressed voluntarily for short periods of time.Common tics include repetitive sniffing or shoulder shrugging.Tics may be single or multiple and transient or chronic.Gilles de la Tourette's syndrome is characterized by chronic multiple tics;its pharmacologic management is discussed at the end of this chapter. Many of the movement disorders have been attributed to disturbances of the basal ganglia,but the precise function of these anatomic structures is not yet fully understood,and it is not possible to relate individual symptoms to involvement at specific sites
Pharmacologic Management of Parkinsonism & Other Movement Disorders Michael J. Aminof , MD, DSc, FRCP INTRODUCTION Several types of abnormal movement are recognized. Tremor consists of a rhythmic oscillatory movement around a joint and is best characterized by its relation to activity. Tremor at rest is characteristic of parkinsonism, when it is often associated with rigidity and an impairment of voluntary activity. Tremor may occur during maintenance of sustained posture (postural tremor) or during movement (intention tremor). A conspicuous postural tremor is the cardinal feature of benign essential or familial tremor. Intention tremor occurs in patients with a lesion of the brainstem or cerebellum, especially when the superior cerebellar peduncle is involved, and may also occur as a manifestation of toxicity from alcohol or certain other drugs. Chorea consists of irregular, unpredictable, involuntary muscle jerks that occur in different parts of the body and impair voluntary activity. In some instances, the proximal muscles of the limbs are most severely affected, and because the abnormal movements are then particularly violent, the term ballismus has been used to describe them. Chorea may be hereditary or may occur as a complication of a number of general medical disorders and of therapy with certain drugs. Abnormal movements may be slow and writhing in character (athetosis) and in some instances are so sustained that they are more properly regarded as abnormal postures (dystonia). Athetosis or dystonia may occur with perinatal brain damage, with focal or generalized cerebral lesions, as an acute complication of certain drugs, as an accompaniment of diverse neurologic disorders, or as an isolated inherited phenomenon of uncertain cause known as idiopathic torsion dystonia or dystonia musculorum deformans. Its physiologic basis is uncertain, and treatment is unsatisfactory. Tics are sudden coordinated abnormal movements that tend to occur repetitively, particularly about the face and head, especially in children, and can be suppressed voluntarily for short periods of time. Common tics include repetitive sniffing or shoulder shrugging. Tics may be single or multiple and transient or chronic. Gilles de la Tourette's syndrome is characterized by chronic multiple tics; its pharmacologic management is discussed at the end of this chapter. Many of the movement disorders have been attributed to disturbances of the basal ganglia, but the precise function of these anatomic structures is not yet fully understood, and it is not possible to relate individual symptoms to involvement at specific sites
PARKINSONISM (PARALYSIS AGITANS) INTRODUCTION Parkinsonism is characterized by a combination of rigidity,bradykinesia,tremor,and postural instability that can occur for a variety of reasons but is usually idiopathic. The pathophysiologic basis of the idiopathic disorder may relate to exposure to some unrecognized neurotoxin or to the occurrence of oxidation reactions with the generation of free radicals.Studies in twins suggest that genetic factors may also be important,especially when the disease occurs in patients under age 50.Parkinson's disease is generally progressive,leading to increasing disability unless effective treatment is provided. The normally high concentration of dopamine in the basal ganglia of the brain is reduced in parkinsonism,and pharmacologic attempts to restore dopaminergic activity with levodopa and dopamine agonists have been successful in alleviating many of the clinical features of the disorder.An alternative but complementary approach has been to restore the normal balance of cholinergic and dopaminergic influences on the basal ganglia with antimuscarinic drugs.The pathophysiologic basis for these therapies is that in idiopathic parkinsonism,dopaminergic neurons in the substantia nigra that normally inhibit the output of GABAergic cells in the corpus striatum are lost(Figure 28-1).(In contrast,Huntington's chorea involves the loss of some cholinergic neurons and an even greater loss of the GABAergic cells that exit the corpus striatum.) Drugs that induce parkinsonian syndromes either are dopamine receptor antagonists or lead to the destruction of the dopaminergic nigrostriatal neurons (eg, 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine [MPTP];see below). Normal Substantia Corpus nigra striatum ⊙ Dopamine Acetyl- GABA choline L Parkinsonism L Huntington's disease
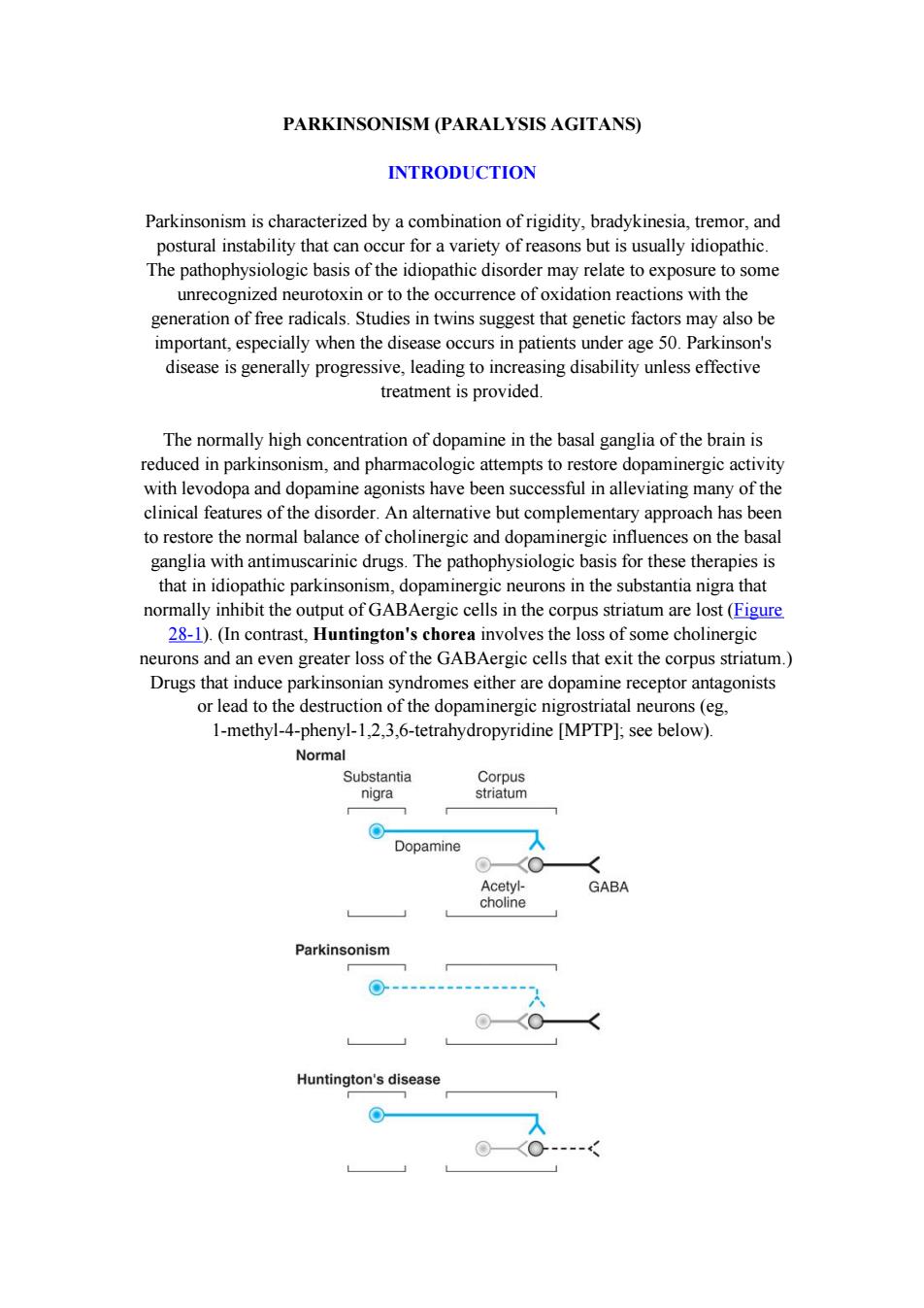
PARKINSONISM (PARALYSIS AGITANS) INTRODUCTION Parkinsonism is characterized by a combination of rigidity, bradykinesia, tremor, and postural instability that can occur for a variety of reasons but is usually idiopathic. The pathophysiologic basis of the idiopathic disorder may relate to exposure to some unrecognized neurotoxin or to the occurrence of oxidation reactions with the generation of free radicals. Studies in twins suggest that genetic factors may also be important, especially when the disease occurs in patients under age 50. Parkinson's disease is generally progressive, leading to increasing disability unless effective treatment is provided. The normally high concentration of dopamine in the basal ganglia of the brain is reduced in parkinsonism, and pharmacologic attempts to restore dopaminergic activity with levodopa and dopamine agonists have been successful in alleviating many of the clinical features of the disorder. An alternative but complementary approach has been to restore the normal balance of cholinergic and dopaminergic influences on the basal ganglia with antimuscarinic drugs. The pathophysiologic basis for these therapies is that in idiopathic parkinsonism, dopaminergic neurons in the substantia nigra that normally inhibit the output of GABAergic cells in the corpus striatum are lost (Figure 28-1). (In contrast, Huntington's chorea involves the loss of some cholinergic neurons and an even greater loss of the GABAergic cells that exit the corpus striatum.) Drugs that induce parkinsonian syndromes either are dopamine receptor antagonists or lead to the destruction of the dopaminergic nigrostriatal neurons (eg, 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine [MPTP]; see below)
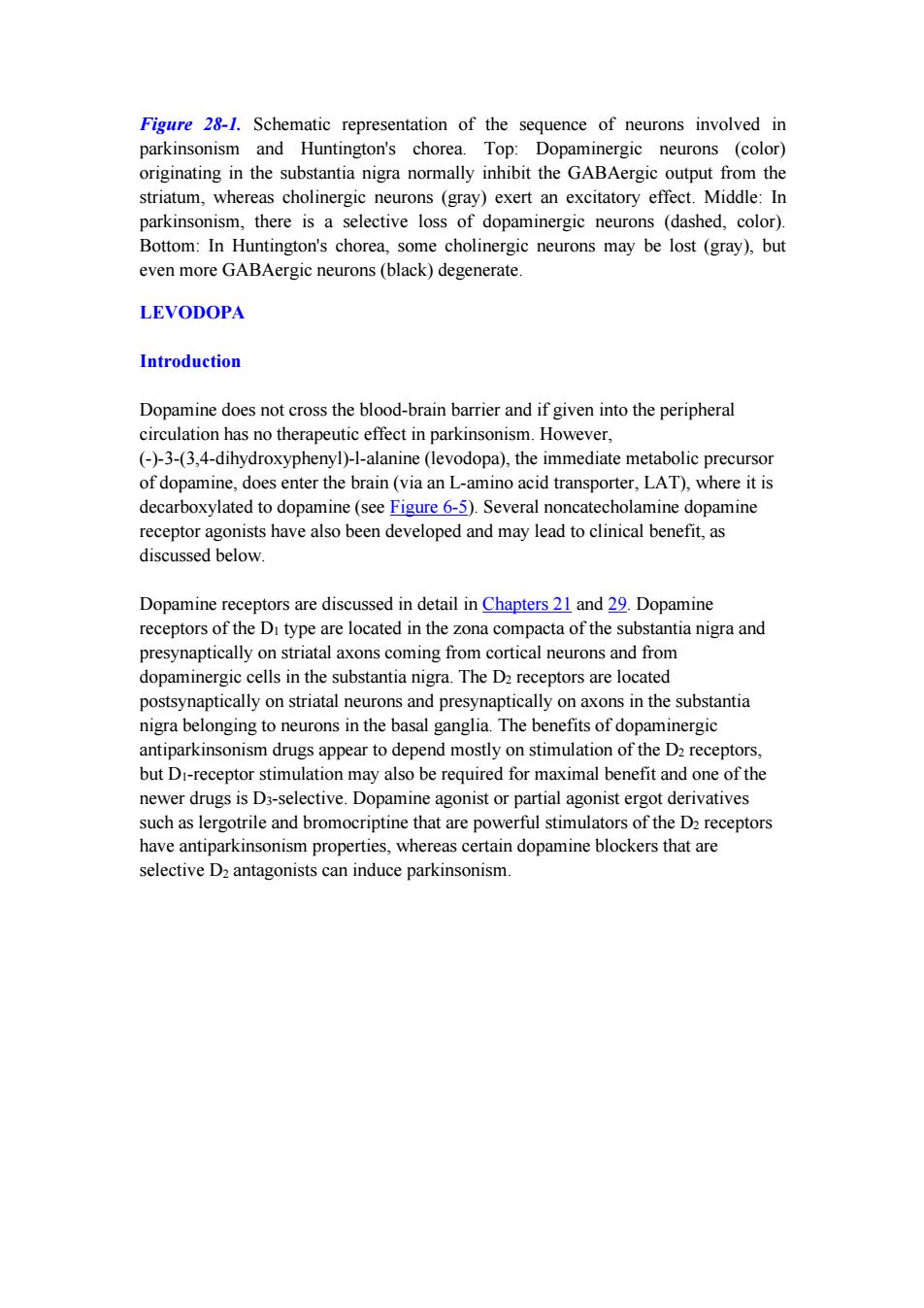
Figure 28-1.Schematic representation of the sequence of neurons involved in parkinsonism and Huntington's chorea.Top:Dopaminergic neurons (color) originating in the substantia nigra normally inhibit the GABAergic output from the striatum,whereas cholinergic neurons (gray)exert an excitatory effect.Middle:In parkinsonism,there is a selective loss of dopaminergic neurons (dashed,color). Bottom:In Huntington's chorea,some cholinergic neurons may be lost (gray),but even more GABAergic neurons(black)degenerate. LEVODOPA Introduction Dopamine does not cross the blood-brain barrier and if given into the peripheral circulation has no therapeutic effect in parkinsonism.However, (-)-3-(3,4-dihydroxyphenyl)-1-alanine (levodopa),the immediate metabolic precursor of dopamine,does enter the brain(via an L-amino acid transporter,LAT),where it is decarboxylated to dopamine(see Figure 6-5).Several noncatecholamine dopamine receptor agonists have also been developed and may lead to clinical benefit,as discussed below. Dopamine receptors are discussed in detail in Chapters 21 and 29.Dopamine receptors of the Di type are located in the zona compacta of the substantia nigra and presynaptically on striatal axons coming from cortical neurons and from dopaminergic cells in the substantia nigra.The D2 receptors are located postsynaptically on striatal neurons and presynaptically on axons in the substantia nigra belonging to neurons in the basal ganglia.The benefits of dopaminergic antiparkinsonism drugs appear to depend mostly on stimulation of the D2 receptors, but Di-receptor stimulation may also be required for maximal benefit and one of the newer drugs is D3-selective.Dopamine agonist or partial agonist ergot derivatives such as lergotrile and bromocriptine that are powerful stimulators of the D2 receptors have antiparkinsonism properties,whereas certain dopamine blockers that are selective D2 antagonists can induce parkinsonism
Figure 28-1. Schematic representation of the sequence of neurons involved in parkinsonism and Huntington's chorea. Top: Dopaminergic neurons (color) originating in the substantia nigra normally inhibit the GABAergic output from the striatum, whereas cholinergic neurons (gray) exert an excitatory effect. Middle: In parkinsonism, there is a selective loss of dopaminergic neurons (dashed, color). Bottom: In Huntington's chorea, some cholinergic neurons may be lost (gray), but even more GABAergic neurons (black) degenerate. LEVODOPA Introduction Dopamine does not cross the blood-brain barrier and if given into the peripheral circulation has no therapeutic effect in parkinsonism. However, (-)-3-(3,4-dihydroxyphenyl)-l-alanine (levodopa), the immediate metabolic precursor of dopamine, does enter the brain (via an L-amino acid transporter, LAT), where it is decarboxylated to dopamine (see Figure 6-5). Several noncatecholamine dopamine receptor agonists have also been developed and may lead to clinical benefit, as discussed below. Dopamine receptors are discussed in detail in Chapters 21 and 29. Dopamine receptors of the D1 type are located in the zona compacta of the substantia nigra and presynaptically on striatal axons coming from cortical neurons and from dopaminergic cells in the substantia nigra. The D2 receptors are located postsynaptically on striatal neurons and presynaptically on axons in the substantia nigra belonging to neurons in the basal ganglia. The benefits of dopaminergic antiparkinsonism drugs appear to depend mostly on stimulation of the D2 receptors, but D1-receptor stimulation may also be required for maximal benefit and one of the newer drugs is D3-selective. Dopamine agonist or partial agonist ergot derivatives such as lergotrile and bromocriptine that are powerful stimulators of the D2 receptors have antiparkinsonism properties, whereas certain dopamine blockers that are selective D2 antagonists can induce parkinsonism
OH NH Tyrosine L-Amino acid decarboxylase Metyrosine Tyrosine hydroxylase OH C=0 HO C-NH H Dopa Tyramine C00H Dopa decarboxylase Dopamine HO B-hydroxylase HO 0 H N-Methyl- Dopamine HO -NH transterase Dopamine B-hydroxylase Octopamine Hydroxylase (from liver) 0 Epinine Norepinephrine Phenylethanolamine-N-methyltransferase Phenylamine- B-hydroxylase HO H Epinephrine Figure 6-5.Biosynthesis of catecholamines.The rate-limiting step,conversion of tyrosine to dopa,can be inhibited by metyrosine(a-methyltyrosine).The alternative pathways shown by the dashed arrows have not been found to be of physiologic significance in humans.However,tyramine and octopamine may accumulate in patients treated with monoamine oxidase inhibitors.(Reproduced,with permission, from Greenspan FS,Gardner DG (editors):Basic and Clinical Endocrinology,7th ed. McGraw-Hill,2003.) Chemistry As discussed in Chapter 6,dopa is the amino acid precursor of dopamine and norepinephrine.Its structure is shown in Figure 28-2.Levodopa is the levorotatory stereoisomer of dopa
Figure 6-5. Biosynthesis of catecholamines. The rate-limiting step, conversion of tyrosine to dopa, can be inhibited by metyrosine (a-methyltyrosine). The alternative pathways shown by the dashed arrows have not been found to be of physiologic significance in humans. However, tyramine and octopamine may accumulate in patients treated with monoamine oxidase inhibitors. (Reproduced, with permission, from Greenspan FS, Gardner DG (editors): Basic and Clinical Endocrinology, 7th ed. McGraw-Hill, 2003.) Chemistry As discussed in Chapter 6, dopa is the amino acid precursor of dopamine and norepinephrine. Its structure is shown in Figure 28-2. Levodopa is the levorotatory stereoisomer of dopa
HO CH2-CH-COOH NH2 HO Dihydroxyphenylalanine (dopa) CH3 HO CH2-C-COOH NH-NH2 HO Carbidopa CH3 CH2一CH一N一CH2一C≡CH CH3 Selegiline C≡N CH2CH3 02N CH=C一C一N ∥ CH2CH3 0 HO OH Entacapone Figure 28-2.Some drugs used in the treatment of parkinsonism. Pharmacokinetics Levodopa is rapidly absorbed from the small intestine,but its absorption depends on the rate of gastric emptying and the pH of the gastric contents.Ingestion of food delays the appearance of levodopa in the plasma.Moreover,certain amino acids from ingested food can compete with the drug for absorption from the gut and for transport
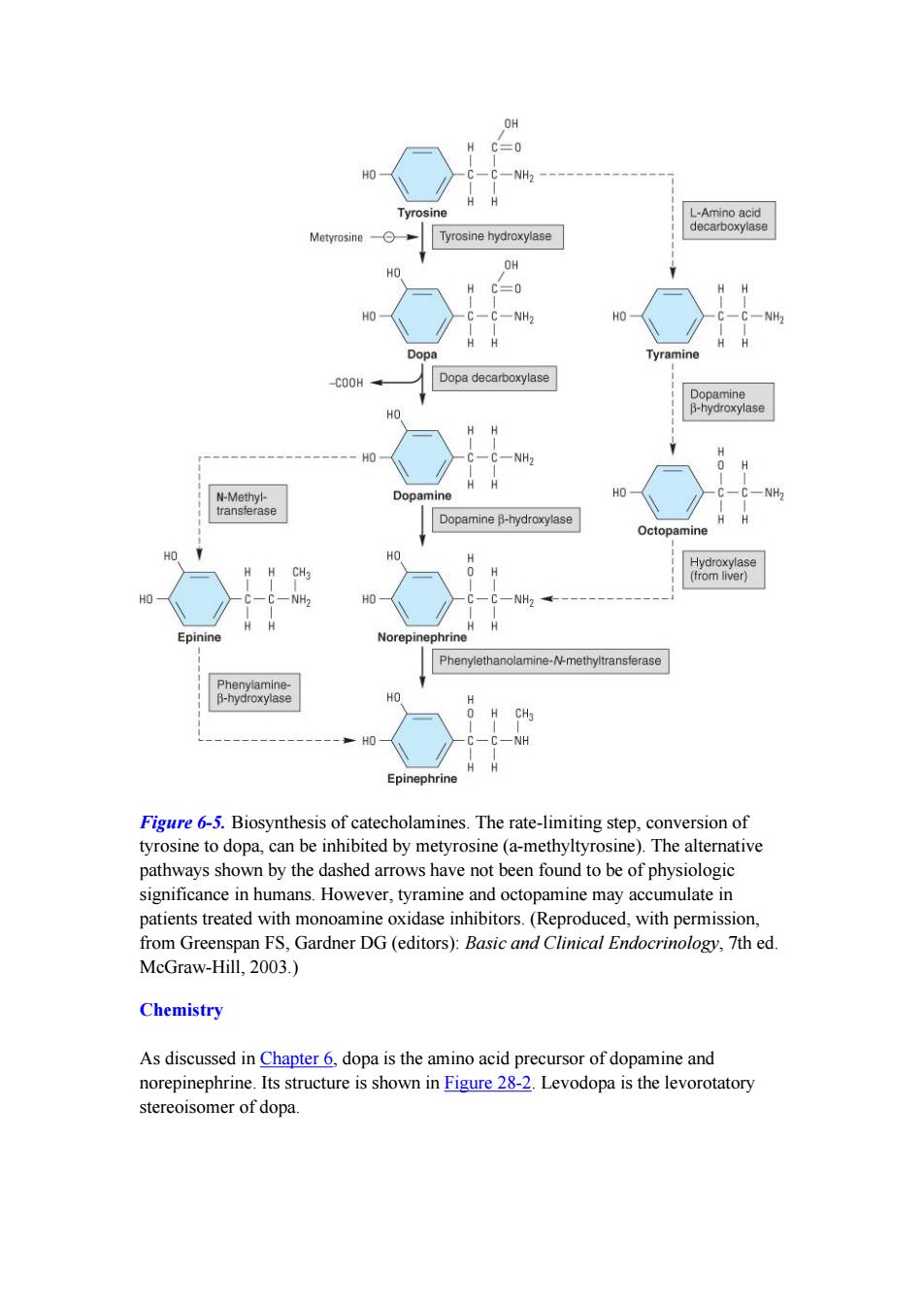
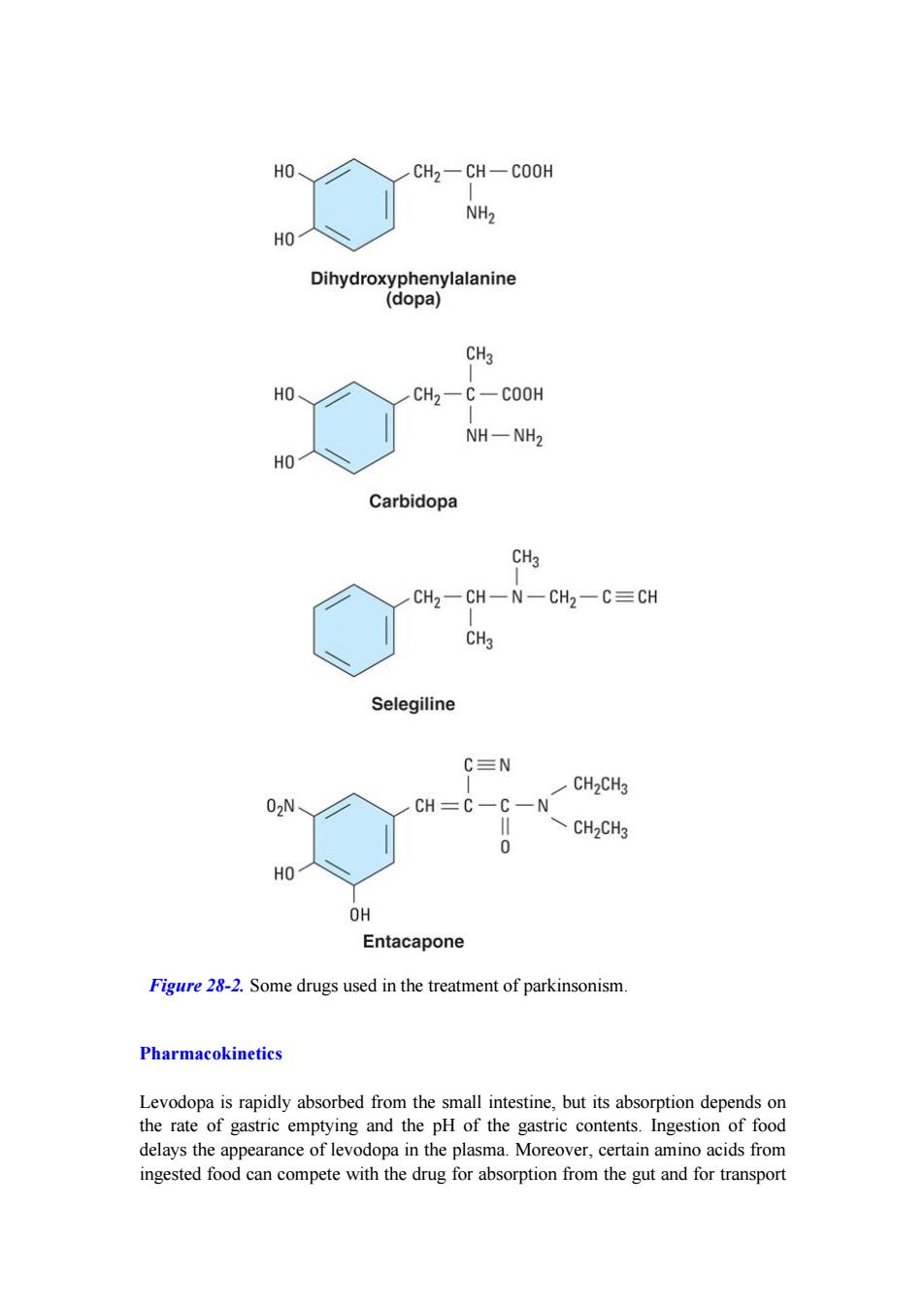
Figure 28-2. Some drugs used in the treatment of parkinsonism. Pharmacokinetics Levodopa is rapidly absorbed from the small intestine, but its absorption depends on the rate of gastric emptying and the pH of the gastric contents. Ingestion of food delays the appearance of levodopa in the plasma. Moreover, certain amino acids from ingested food can compete with the drug for absorption from the gut and for transport