smooth muscle,as well as smooth muscle in the prostate,due to blockade of a receptors.Prazosin is extensively metabolized in humans;because of metabolic degradation by the liver,only about 50%of the drug is available after oral administration.The half-life is normally about 3 hours. Terazosin is another reversible a-selective antagonist that is effective in hypertension(Chapter 11);it is also approved for use in men with urinary symptoms due to benign prostatic hyperplasia(BPH).Terazosin has high bioavailability but is extensively metabolized in the liver,with only a small fraction of unchanged drug excreted in the urine.The half-life of terazosin is 9-12 hours. Doxazosin is efficacious in the treatment of hypertension and BPH.It differs from prazosin and terazosin in having a longer half-life of about 22 hours.It has moderate bioavailability and is extensively metabolized,with very little parent drug excreted in urine or feces.Doxazosin has active metabolites,although their contribution to the drug's effects is probably small. Tamsulosin is a competitive ai antagonist with a structure quite different from that of most other ai-receptor blockers.It has high bioavailability and a long half-life of 9-15 hours.It is metabolized extensively in the liver.Tamsulosin has higher affinity for ai and aiD receptors than for the aiB subtype.Evidence suggests that tamsulosin has relatively greater potency in inhibiting contraction in prostate smooth muscle versus vascular smooth muscle compared with other ai-selective antagonists.The drug's efficacy in BPH suggests that the aiA subtype may be the most important a subtype mediating prostate smooth muscle contraction.Furthermore,compared with other antagonists,tamsulosin has less effect on standing blood pressure in patients. Nevertheless,caution is appropriate in using any a antagonist in patients with diminished sympathetic nervous system function. OTHER ALPHA-ADRENOCEPTOR ANTAGONISTS Alfuzosin is an a-selective quinazoline derivative that is approved for use in BPH.It has a bioavailability of about 60%,is extensively metabolized,and has an elimination half-life of about 5 hours.Indoramin is another a-selective antagonist that also has efficacy as an antihypertensive.Urapidil is an a antagonist (its primary effect)that also has weak a2-agonist and 5-HTIA-agonist actions and weak antagonist action at b receptors.It is used in Europe as an antihypertensive agent and for benign prostatic hyperplasia.Labetalol has both a-selective and b-antagonistic effects;it is discussed below.Neuroleptic drugs such as chlorpromazine and haloperidol are potent dopamine receptor antagonists but are also antagonists at a receptors.Their antagonism of a receptors probably contributes to some of their adverse effects, particularly hypotension.Similarly,the antidepressant trazodone has the capacity to block ai receptors
smooth muscle, as well as smooth muscle in the prostate, due to blockade of a1 receptors. Prazosin is extensively metabolized in humans; because of metabolic degradation by the liver, only about 50% of the drug is available after oral administration. The half-life is normally about 3 hours. Terazosin is another reversible a1-selective antagonist that is effective in hypertension (Chapter 11); it is also approved for use in men with urinary symptoms due to benign prostatic hyperplasia (BPH). Terazosin has high bioavailability but is extensively metabolized in the liver, with only a small fraction of unchanged drug excreted in the urine. The half-life of terazosin is 9-12 hours. Doxazosin is efficacious in the treatment of hypertension and BPH. It differs from prazosin and terazosin in having a longer half-life of about 22 hours. It has moderate bioavailability and is extensively metabolized, with very little parent drug excreted in urine or feces. Doxazosin has active metabolites, although their contribution to the drug's effects is probably small. Tamsulosin is a competitive a1 antagonist with a structure quite different from that of most other a1-receptor blockers. It has high bioavailability and a long half-life of 9-15 hours. It is metabolized extensively in the liver. Tamsulosin has higher affinity for a1A and a1D receptors than for the a1B subtype. Evidence suggests that tamsulosin has relatively greater potency in inhibiting contraction in prostate smooth muscle versus vascular smooth muscle compared with other a1-selective antagonists. The drug's efficacy in BPH suggests that the a1A subtype may be the most important a subtype mediating prostate smooth muscle contraction. Furthermore, compared with other antagonists, tamsulosin has less effect on standing blood pressure in patients. Nevertheless, caution is appropriate in using any a antagonist in patients with diminished sympathetic nervous system function. OTHER ALPHA-ADRENOCEPTOR ANTAGONISTS Alfuzosin is an a1-selective quinazoline derivative that is approved for use in BPH. It has a bioavailability of about 60%, is extensively metabolized, and has an elimination half-life of about 5 hours. Indoramin is another a1-selective antagonist that also has efficacy as an antihypertensive. Urapidil is an a1 antagonist (its primary effect) that also has weak a2-agonist and 5-HT1A-agonist actions and weak antagonist action at b1 receptors. It is used in Europe as an antihypertensive agent and for benign prostatic hyperplasia. Labetalol has both a1-selective and b-antagonistic effects; it is discussed below. Neuroleptic drugs such as chlorpromazine and haloperidol are potent dopamine receptor antagonists but are also antagonists at a receptors. Their antagonism of a receptors probably contributes to some of their adverse effects, particularly hypotension. Similarly, the antidepressant trazodone has the capacity to block a1 receptors
Yohimbine,an indole alkaloid,is an az-selective antagonist.It has no established clinical role.Theoretically,it could be useful in autonomic insufficiency by promoting neurotransmitter release through blockade of presynaptic a2 receptors.It has been suggested that yohimbine improves male sexual function;however,evidence for this effect in humans is limited.Yohimbine can abruptly reverse the antihypertensive effects of an az-adrenoceptor agonist such as clonidine%a potentially serious adverse drug interaction. II.CLINICAL PHARMACOLOGY OF THE ALPHA-RECEPTOR-BLOCKING DRUGS Pheochromocytoma The major clinical use of both phenoxybenzamine and phentolamine is in the management of pheochromocytoma.This tumor is usually found in the adrenal medulla;it typically releases a mixture of epinephrine and norepinephrine.Patients have many symptoms and signs of catecholamine excess,including intermittent or sustained hypertension,headaches,palpitations,and increased sweating. The diagnosis of pheochromocytoma is usually made on the basis of chemical assay of circulating catecholamines and urinary excretion of catecholamine metabolites, especially 3-hydroxy-4-methoxymandelic acid,metanephrine,and normetanephrine (see Chapter 6).Measurement of plasma metanephrines is also an effective diagnostic tool.A variety of diagnostic techniques are available to localize a pheochromocytoma diagnosed biochemically,including CT and MRI scans as well as scanning with various radioisotopes. Unavoidable release of stored catecholamines sometimes occurs during operative manipulation of pheochromocytoma;the resulting hypertension may be controlled with phentolamine or nitroprusside.Nitroprusside has many advantages,particularly since its effects can be more readily titrated and it has a shorter duration of action. Alpha-receptor antagonists are most useful in the preoperative management of patients with pheochromocytoma(Figure 10-4).Administration of phenoxybenzamine in the preoperative period will help control hypertension and will tend to reverse chronic changes resulting from excessive catecholamine secretion such as plasma volume contraction,if present.Furthermore,the patient's operative course may be simplified.Oral doses of 10-20 mg/d can be increased at intervals of several days until hypertension is controlled.Some physicians give phenoxybenzamine to patients with pheochromocytoma for 1-3 weeks before surgery.Other surgeons prefer to operate on patients in the absence of treatment with phenoxybenzamine,counting on modern anesthetic techniques to control blood pressure and heart rate during surgery. Phenoxybenzamine can be very useful in the chronic treatment of inoperable or
Yohimbine, an indole alkaloid, is an a2-selective antagonist. It has no established clinical role. Theoretically, it could be useful in autonomic insufficiency by promoting neurotransmitter release through blockade of presynaptic a2 receptors. It has been suggested that yohimbine improves male sexual function; however, evidence for this effect in humans is limited. Yohimbine can abruptly reverse the antihypertensive effects of an a2-adrenoceptor agonist such as clonidine¾a potentially serious adverse drug interaction. II. CLINICAL PHARMACOLOGY OF THE ALPHA-RECEPTOR-BLOCKING DRUGS Pheochromocytoma The major clinical use of both phenoxybenzamine and phentolamine is in the management of pheochromocytoma. This tumor is usually found in the adrenal medulla; it typically releases a mixture of epinephrine and norepinephrine. Patients have many symptoms and signs of catecholamine excess, including intermittent or sustained hypertension, headaches, palpitations, and increased sweating. The diagnosis of pheochromocytoma is usually made on the basis of chemical assay of circulating catecholamines and urinary excretion of catecholamine metabolites, especially 3-hydroxy-4-methoxymandelic acid, metanephrine, and normetanephrine (see Chapter 6). Measurement of plasma metanephrines is also an effective diagnostic tool. A variety of diagnostic techniques are available to localize a pheochromocytoma diagnosed biochemically, including CT and MRI scans as well as scanning with various radioisotopes. Unavoidable release of stored catecholamines sometimes occurs during operative manipulation of pheochromocytoma; the resulting hypertension may be controlled with phentolamine or nitroprusside. Nitroprusside has many advantages, particularly since its effects can be more readily titrated and it has a shorter duration of action. Alpha-receptor antagonists are most useful in the preoperative management of patients with pheochromocytoma (Figure 10-4). Administration of phenoxybenzamine in the preoperative period will help control hypertension and will tend to reverse chronic changes resulting from excessive catecholamine secretion such as plasma volume contraction, if present. Furthermore, the patient's operative course may be simplified. Oral doses of 10-20 mg/d can be increased at intervals of several days until hypertension is controlled. Some physicians give phenoxybenzamine to patients with pheochromocytoma for 1-3 weeks before surgery. Other surgeons prefer to operate on patients in the absence of treatment with phenoxybenzamine, counting on modern anesthetic techniques to control blood pressure and heart rate during surgery. Phenoxybenzamine can be very useful in the chronic treatment of inoperable or
metastatic pheochromocytoma.Although there is less experience with alternative drugs,hypertension in patients with pheochromocytoma may also respond to reversible a-selective antagonists or to conventional calcium channel antagonists. Beta-receptor antagonists may be required after a-receptor blockade has been instituted to reverse the cardiac effects of excessive catecholamines.Beta antagonists should not be used prior to establishing effective a-receptor blockade,since unopposed b-receptor blockade could theoretically cause blood pressure elevation from increased vasoconstriction. Pheochromocytoma is rarely treated with metyrosine(a-methyltyrosine),the a-methyl analog of tyrosine.This agent is a competitive inhibitor of tyrosine hydroxylase and interferes with synthesis of dopamine,norepinephrine,and epinephrine(see Figure 6-5).Metyrosine is especially useful in symptomatic patients with inoperable or metastatic pheochromocytoma. HO Tyrosine L-Amino acid decarboxylase Metyrosine- Tyrosine hydroxylase HO OH HO -C-NH2 HO Dopa Tyramine Dopa decarboxylase Dopamine HO B-hydroxylase H HO NH N-Methyl- Dopamine H0- transferase Dopamine B-hydroxylase Octopamine Hydroxylase CH (from liver) HO Epinine Norepinephrine Phenylethanolamine-N-methyltransterase Phenylamine- B-hydroxylase HO Epinephrine
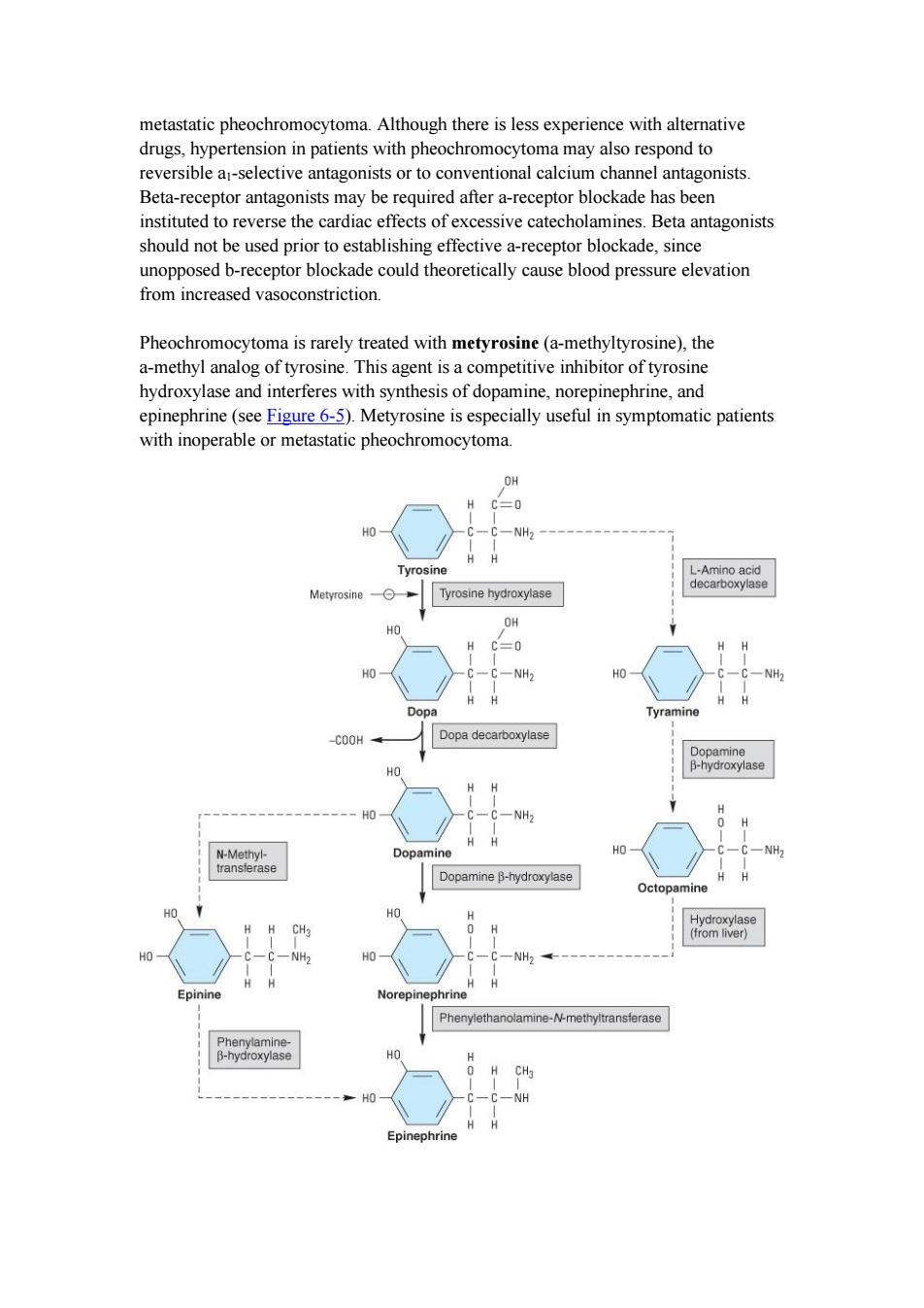
metastatic pheochromocytoma. Although there is less experience with alternative drugs, hypertension in patients with pheochromocytoma may also respond to reversible a1-selective antagonists or to conventional calcium channel antagonists. Beta-receptor antagonists may be required after a-receptor blockade has been instituted to reverse the cardiac effects of excessive catecholamines. Beta antagonists should not be used prior to establishing effective a-receptor blockade, since unopposed b-receptor blockade could theoretically cause blood pressure elevation from increased vasoconstriction. Pheochromocytoma is rarely treated with metyrosine (a-methyltyrosine), the a-methyl analog of tyrosine. This agent is a competitive inhibitor of tyrosine hydroxylase and interferes with synthesis of dopamine, norepinephrine, and epinephrine (see Figure 6-5). Metyrosine is especially useful in symptomatic patients with inoperable or metastatic pheochromocytoma
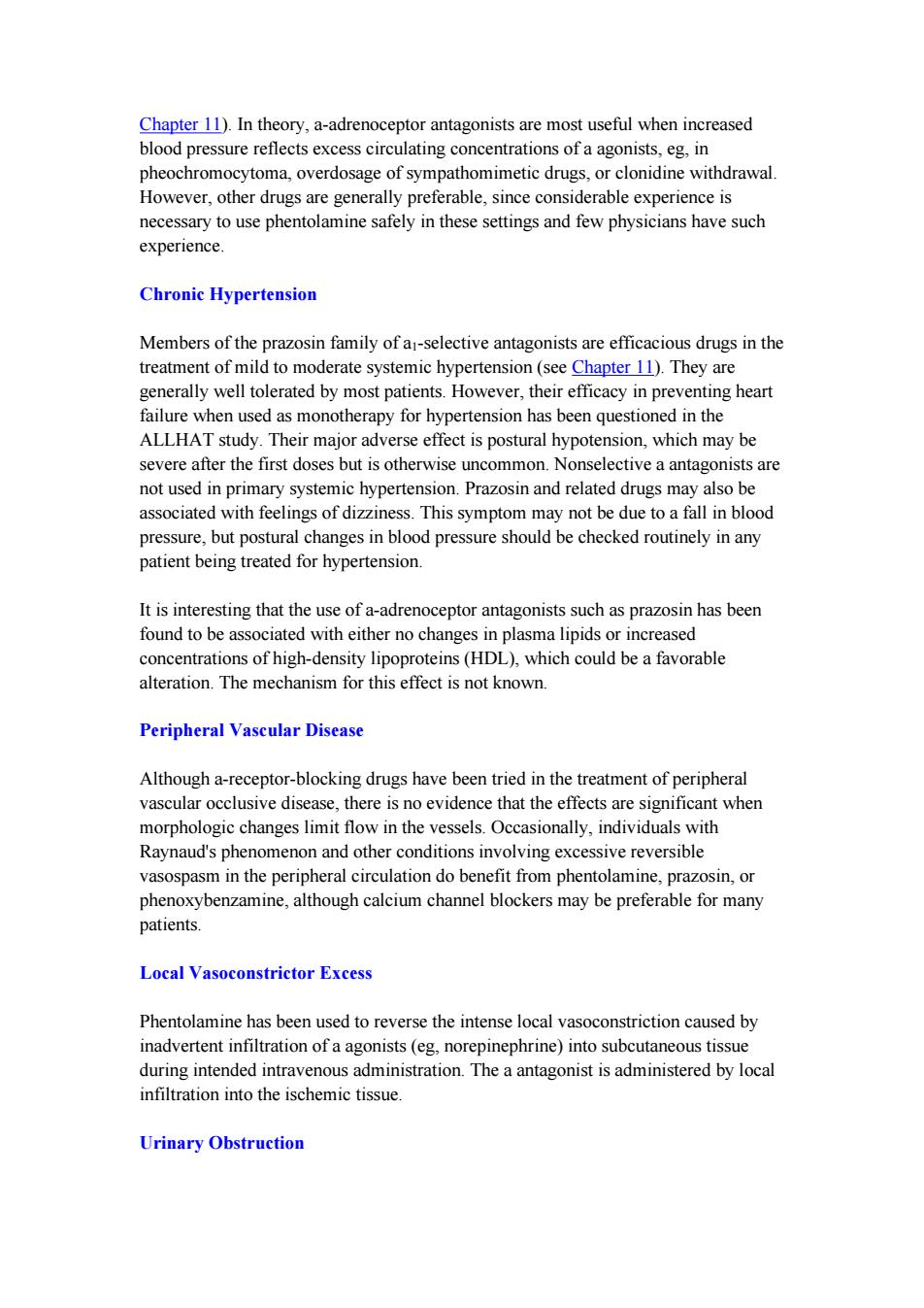
240 220 o-o Supine Standing 200 180 160 ww) 140 120 100 60 0 Dibenzyline 0 p/bw 40 20 1 23456789101112131415 Weeks Figure 6-5.Biosynthesis of catecholamines.The rate-limiting step,conversion of tyrosine to dopa,can be inhibited by metyrosine(a-methyltyrosine).The alternative pathways shown by the dashed arrows have not been found to be of physiologic significance in humans.However,tyramine and octopamine may accumulate in patients treated with monoamine oxidase inhibitors.(Reproduced,with permission, from Greenspan FS,Gardner DG (editors):Basic and Clinical Endocrinology,7th ed. McGraw-Hill,2003.) Figure 10-4.Effects of phenoxybenzamine (Dibenzyline)on blood pressure in a patient with pheochromocytoma.Dosage of the drug was begun in the third week as shown by the shaded bar.Supine systolic and diastolic pressures are indicated by the circles,the standing pressures by triangles and the hatched area.Note that the a-blocking drug dramatically reduced blood pressure.The reduction in orthostatic hypotension,which was marked before treatment,is probably due to normalization of blood volume,a variable that is sometimes markedly reduced in patients with longstanding pheochromocytoma-induced hypertension.(Redrawn and reproduced, with permission,from Engelman E,Sjoerdsma A:Chronic medical therapy for pheochromocytoma.Ann Intern Med 1961:61:229.) Hypertensive Emergencies The a-adrenoceptor antagonist drugs have limited application in the management of hypertensive emergencies,although labetalol has been used in this setting(see
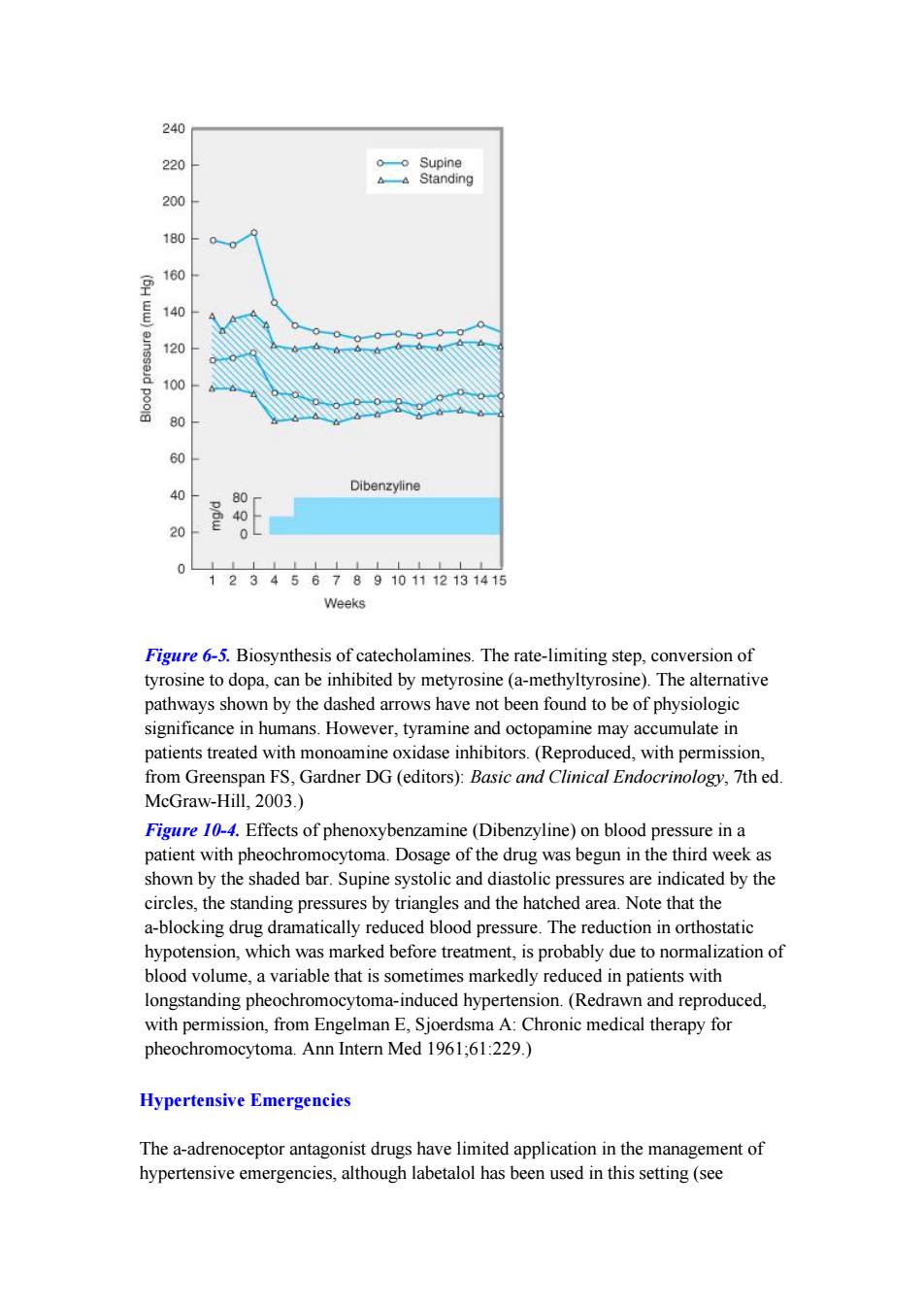
Figure 6-5. Biosynthesis of catecholamines. The rate-limiting step, conversion of tyrosine to dopa, can be inhibited by metyrosine (a-methyltyrosine). The alternative pathways shown by the dashed arrows have not been found to be of physiologic significance in humans. However, tyramine and octopamine may accumulate in patients treated with monoamine oxidase inhibitors. (Reproduced, with permission, from Greenspan FS, Gardner DG (editors): Basic and Clinical Endocrinology, 7th ed. McGraw-Hill, 2003.) Figure 10-4. Effects of phenoxybenzamine (Dibenzyline) on blood pressure in a patient with pheochromocytoma. Dosage of the drug was begun in the third week as shown by the shaded bar. Supine systolic and diastolic pressures are indicated by the circles, the standing pressures by triangles and the hatched area. Note that the a-blocking drug dramatically reduced blood pressure. The reduction in orthostatic hypotension, which was marked before treatment, is probably due to normalization of blood volume, a variable that is sometimes markedly reduced in patients with longstanding pheochromocytoma-induced hypertension. (Redrawn and reproduced, with permission, from Engelman E, Sjoerdsma A: Chronic medical therapy for pheochromocytoma. Ann Intern Med 1961;61:229.) Hypertensive Emergencies The a-adrenoceptor antagonist drugs have limited application in the management of hypertensive emergencies, although labetalol has been used in this setting (see
Chapter 11).In theory,a-adrenoceptor antagonists are most useful when increased blood pressure reflects excess circulating concentrations of a agonists,eg,in pheochromocytoma,overdosage of sympathomimetic drugs,or clonidine withdrawal. However,other drugs are generally preferable,since considerable experience is necessary to use phentolamine safely in these settings and few physicians have such experience Chronic Hypertension Members of the prazosin family of a-selective antagonists are efficacious drugs in the treatment of mild to moderate systemic hypertension(see Chapter 11).They are generally well tolerated by most patients.However,their efficacy in preventing heart failure when used as monotherapy for hypertension has been questioned in the ALLHAT study.Their major adverse effect is postural hypotension,which may be severe after the first doses but is otherwise uncommon.Nonselective a antagonists are not used in primary systemic hypertension.Prazosin and related drugs may also be associated with feelings of dizziness.This symptom may not be due to a fall in blood pressure,but postural changes in blood pressure should be checked routinely in any patient being treated for hypertension. It is interesting that the use of a-adrenoceptor antagonists such as prazosin has been found to be associated with either no changes in plasma lipids or increased concentrations of high-density lipoproteins(HDL),which could be a favorable alteration.The mechanism for this effect is not known. Peripheral Vascular Disease Although a-receptor-blocking drugs have been tried in the treatment of peripheral vascular occlusive disease,there is no evidence that the effects are significant when morphologic changes limit flow in the vessels.Occasionally,individuals with Raynaud's phenomenon and other conditions involving excessive reversible vasospasm in the peripheral circulation do benefit from phentolamine,prazosin,or phenoxybenzamine,although calcium channel blockers may be preferable for many patients Local Vasoconstrictor Excess Phentolamine has been used to reverse the intense local vasoconstriction caused by inadvertent infiltration of a agonists(eg,norepinephrine)into subcutaneous tissue during intended intravenous administration.The a antagonist is administered by local infiltration into the ischemic tissue. Urinary Obstruction
Chapter 11). In theory, a-adrenoceptor antagonists are most useful when increased blood pressure reflects excess circulating concentrations of a agonists, eg, in pheochromocytoma, overdosage of sympathomimetic drugs, or clonidine withdrawal. However, other drugs are generally preferable, since considerable experience is necessary to use phentolamine safely in these settings and few physicians have such experience. Chronic Hypertension Members of the prazosin family of a1-selective antagonists are efficacious drugs in the treatment of mild to moderate systemic hypertension (see Chapter 11). They are generally well tolerated by most patients. However, their efficacy in preventing heart failure when used as monotherapy for hypertension has been questioned in the ALLHAT study. Their major adverse effect is postural hypotension, which may be severe after the first doses but is otherwise uncommon. Nonselective a antagonists are not used in primary systemic hypertension. Prazosin and related drugs may also be associated with feelings of dizziness. This symptom may not be due to a fall in blood pressure, but postural changes in blood pressure should be checked routinely in any patient being treated for hypertension. It is interesting that the use of a-adrenoceptor antagonists such as prazosin has been found to be associated with either no changes in plasma lipids or increased concentrations of high-density lipoproteins (HDL), which could be a favorable alteration. The mechanism for this effect is not known. Peripheral Vascular Disease Although a-receptor-blocking drugs have been tried in the treatment of peripheral vascular occlusive disease, there is no evidence that the effects are significant when morphologic changes limit flow in the vessels. Occasionally, individuals with Raynaud's phenomenon and other conditions involving excessive reversible vasospasm in the peripheral circulation do benefit from phentolamine, prazosin, or phenoxybenzamine, although calcium channel blockers may be preferable for many patients. Local Vasoconstrictor Excess Phentolamine has been used to reverse the intense local vasoconstriction caused by inadvertent infiltration of a agonists (eg, norepinephrine) into subcutaneous tissue during intended intravenous administration. The a antagonist is administered by local infiltration into the ischemic tissue. Urinary Obstruction