Antidepressant Agents William Z.Potter,MD,PhD,Leo E.Hollister,MD* Introduction Major depression is one of the most common psychiatric disorders.At any given moment,about 3-5%of the population is depressed(point prevalence),and an estimated 10%of people may become depressed during their lives(lifetime prevalence).The symptoms of depression are often subtle and unrecognized both by patients and by physicians.Patients with vague complaints that resist explanation as manifestations of somatic disorders and those who might be simplistically described as "neurotic"should be suspected of being depressed. Depression is a heterogeneous disorder that has been characterized and classified in a variety of ways.According to the American Psychiatric Association's modified fourth edition (2000)of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR),several diagnoses of affective disorders are possible.Major depression and dysthymia(minor)are pure depressive syndromes,whereas bipolar disorder and cyclothymic disorder signify depression in association with mania.A simplified classification based on presumed origin is as follows:(1)brief reactive or secondary depression(most common),occurring in response to real stimuli such as grief,illness, etc;(2)melancholic and recurrent depression,a genetically determined biochemical disorder manifested by an inability to experience ordinary pleasure or to cope with ordinary life events;and (3)depression associated with bipolar affective (manic-depressive)disorder.Because safe antidepressants are now available,almost any individual with several symptoms of depression that persist beyond a few weeks is a candidate for pharmacologic treatment.Intensive efforts to formalize guidelines for the treatment of depression have been pursued for more than a decade,resulting in guidelines from the American Psychiatric Association,the Agency for Health Care Policy and Research,and the World Federation of Societies of Biological Psychiatry. Pharmacologic treatment is emphasized,although a continuing role for electroconvulsive therapy for delusional or severe forms of life-threatening depression is also noted. *Deceased. The Pathogenesis of Major Depression:The Amine Hypothesis and Subsequent Developments Soon after the introduction of reserpine in the early 1950s,it became apparent that the drug could induce depression.Studies revealed that the principal mechanism of action of reserpine was to inhibit the neuronal storage of amine neurotransmitters such as serotonin and norepinephrine.Reserpine induced depression and depleted stores of amine neurotransmitters;therefore,it was reasoned,depression must be associated with decreased functional amine-dependent synaptic transmission.This idea provided
Antidepressant Agents ¾ William Z. Potter, MD, PhD, & Leo E. Hollister, MD* Introduction Major depression is one of the most common psychiatric disorders. At any given moment, about 3-5% of the population is depressed (point prevalence), and an estimated 10% of people may become depressed during their lives (lifetime prevalence). The symptoms of depression are often subtle and unrecognized both by patients and by physicians. Patients with vague complaints that resist explanation as manifestations of somatic disorders and those who might be simplistically described as "neurotic" should be suspected of being depressed. Depression is a heterogeneous disorder that has been characterized and classified in a variety of ways. According to the American Psychiatric Association's modified fourth edition (2000) of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR), several diagnoses of affective disorders are possible. Major depression and dysthymia (minor) are pure depressive syndromes, whereas bipolar disorder and cyclothymic disorder signify depression in association with mania. A simplified classification based on presumed origin is as follows: (1) brief reactive or secondary depression (most common), occurring in response to real stimuli such as grief, illness, etc; (2) melancholic and recurrent depression, a genetically determined biochemical disorder manifested by an inability to experience ordinary pleasure or to cope with ordinary life events; and (3) depression associated with bipolar affective (manic-depressive) disorder. Because safe antidepressants are now available, almost any individual with several symptoms of depression that persist beyond a few weeks is a candidate for pharmacologic treatment. Intensive efforts to formalize guidelines for the treatment of depression have been pursued for more than a decade, resulting in guidelines from the American Psychiatric Association, the Agency for Health Care Policy and Research, and the World Federation of Societies of Biological Psychiatry. Pharmacologic treatment is emphasized, although a continuing role for electroconvulsive therapy for delusional or severe forms of life-threatening depression is also noted. *Deceased. The Pathogenesis of Major Depression: The Amine Hypothesis and Subsequent Developments Soon after the introduction of reserpine in the early 1950s, it became apparent that the drug could induce depression. Studies revealed that the principal mechanism of action of reserpine was to inhibit the neuronal storage of amine neurotransmitters such as serotonin and norepinephrine. Reserpine induced depression and depleted stores of amine neurotransmitters; therefore, it was reasoned, depression must be associated with decreased functional amine-dependent synaptic transmission. This idea provided
the basis for what became known as the amine hypothesis of depression.By extension, drugs that increased amine function in appropriate synaptic areas would relieve depression.A major puzzle in applying this hypothesis was the fact that although the pharmacologic actions of both tricyclic and monoamine oxidase(MAO)inhibitor classes of antidepressants are prompt,the clinical effects require weeks to become manifest.Attempts have been made to explain this observation by invoking slow compensatory responses to the initial blockade of amine reuptake or MAO inhibition (see below). Current brain imaging and biochemical studies in patients do not support a single biologic abnormality as common to most depressions.Rather,prevailing hypotheses emphasize an underlying role for several brain circuits that have a propensity to become dysfunctional,especially following certain stressors,in individuals with a range of genetic predispositions.It is likely that several pathophysiologic processes will ultimately be identified to account for the presentation of what is now termed major depression. Nevertheless,the amine hypothesis has provided the major experimental models for the discovery of new antidepressant drugs.As a result,all currently available antidepressants,except bupropion,are classified as having their primary actions on the metabolism,reuptake,or selective receptor antagonism of serotonin, norepinephrine,or both. I.BASIC PHARMACOLOGY OF ANTIDEPRESSANTS Chemistry A variety of chemical structures have been found to have antidepressant activity.With the exception of bupropion,however,the core antidepressant action of even the newest agents derives from mechanisms proposed for antidepressants that were introduced four decades ago. A.TRICYCLIC ANTIDEPRESSANTS (TCAS) Tricyclic antidepressants%so called because of the characteristic three-ring nucleus (Figure 30-1)have been used clinically for four decades.They closely resemble the phenothiazines chemically and,to a lesser extent,pharmacologically.Like the phenothiazines,tricyclics were first thought to be useful as antihistamines with sedative properties.The discovery of their antidepressant properties was a fortuitous clinical observation.Imipramine and amitriptyline are the prototypical drugs of the class as mixed norepinephrine and serotonin uptake inhibitors,although they also have several other effects. B.SECOND-GENERATION AND SUBSEQUENT AGENTS
the basis for what became known as the amine hypothesis of depression. By extension, drugs that increased amine function in appropriate synaptic areas would relieve depression. A major puzzle in applying this hypothesis was the fact that although the pharmacologic actions of both tricyclic and monoamine oxidase (MAO) inhibitor classes of antidepressants are prompt, the clinical effects require weeks to become manifest. Attempts have been made to explain this observation by invoking slow compensatory responses to the initial blockade of amine reuptake or MAO inhibition (see below). Current brain imaging and biochemical studies in patients do not support a single biologic abnormality as common to most depressions. Rather, prevailing hypotheses emphasize an underlying role for several brain circuits that have a propensity to become dysfunctional, especially following certain stressors, in individuals with a range of genetic predispositions. It is likely that several pathophysiologic processes will ultimately be identified to account for the presentation of what is now termed major depression. Nevertheless, the amine hypothesis has provided the major experimental models for the discovery of new antidepressant drugs. As a result, all currently available antidepressants, except bupropion, are classified as having their primary actions on the metabolism, reuptake, or selective receptor antagonism of serotonin, norepinephrine, or both. I. BASIC PHARMACOLOGY OF ANTIDEPRESSANTS Chemistry A variety of chemical structures have been found to have antidepressant activity. With the exception of bupropion, however, the core antidepressant action of even the newest agents derives from mechanisms proposed for antidepressants that were introduced four decades ago. A. TRICYCLIC ANTIDEPRESSANTS (TCAS) Tricyclic antidepressants¾so called because of the characteristic three-ring nucleus (Figure 30-1) have been used clinically for four decades. They closely resemble the phenothiazines chemically and, to a lesser extent, pharmacologically. Like the phenothiazines, tricyclics were first thought to be useful as antihistamines with sedative properties. The discovery of their antidepressant properties was a fortuitous clinical observation. Imipramine and amitriptyline are the prototypical drugs of the class as mixed norepinephrine and serotonin uptake inhibitors, although they also have several other effects. B. SECOND-GENERATION AND SUBSEQUENT AGENTS
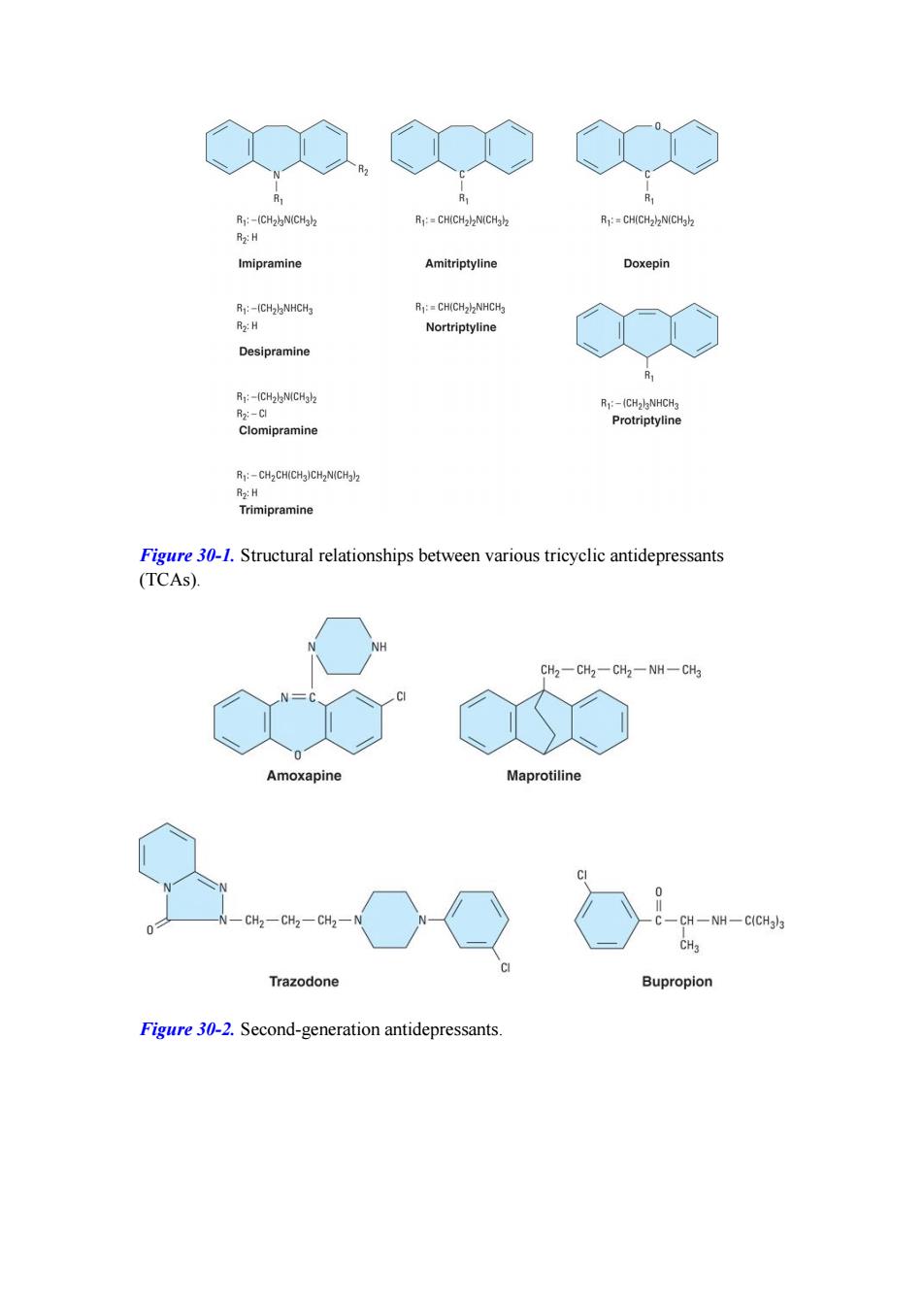
Between 1980 and 2005,thirteen structurally unique antidepressants and one isomeric variation were introduced.The agents classified as second generation and available for clinical use in the USA are shown in Figure 30-2.Amoxapine and maprotiline resemble the structure of the tricyclic agents,whereas trazodone and bupropion are distinctive.Newer,third generation drugs include venlafaxine,mirtazapine, nefazodone,and duloxetine.The structures of these compounds are shown in Figure 30-3.Six additional agents that work mainly through serotonin uptake inhibition are classified together in the following section. C.SELECTIVE SEROTONIN REUPTAKE INHIBITORS (SSRIS) Search for molecules with greater selectivity for the serotonin transporter led to the introduction of fluoxetine%an effective and more selective antidepressant with minimal autonomic toxicity.Since that time,four more SSRIs have been introduced as well as the active enantiomeric form of one,(S)-citalopram.All are structurally distinct from the tricyclic molecules(Figure 30-4).These drugs have fewer adverse effects than the tricyclics and have become very popular. D.MONOAMINE OXIDASE (MAO)INHIBITORS MAO inhibitors may be classified as hydrazides,exemplified by the C-N-N moiety, as is the case with phenelzine and isocarboxazid(no longer marketed);or nonhydrazides,which lack such a moiety,as with tranylcypromine(Figure 30-5). Tranylcypromine closely resembles dextroamphetamine,which is itself a weak inhibitor of MAO.Tranylcypromine retains some of the sympathomimetic characteristics of the amphetamines.The hydrazides appear to combine irreversibly with the enzyme,whereas tranylcypromine has a prolonged duration of effect even though it is not bound irreversibly.These older MAO inhibitors are nonselective inhibitors of both MAO-A and MAO-B.Selegiline,an MAO inhibitor used in Parkinson's disease that is selective for MAO-B at low doses but less selective at higher doses,has been approved for the treatment of major depression
Between 1980 and 2005, thirteen structurally unique antidepressants and one isomeric variation were introduced. The agents classified as second generation and available for clinical use in the USA are shown in Figure 30-2. Amoxapine and maprotiline resemble the structure of the tricyclic agents, whereas trazodone and bupropion are distinctive. Newer, third generation drugs include venlafaxine, mirtazapine, nefazodone, and duloxetine. The structures of these compounds are shown in Figure 30-3. Six additional agents that work mainly through serotonin uptake inhibition are classified together in the following section. C. SELECTIVE SEROTONIN REUPTAKE INHIBITORS (SSRIS) Search for molecules with greater selectivity for the serotonin transporter led to the introduction of fluoxetine¾an effective and more selective antidepressant with minimal autonomic toxicity. Since that time, four more SSRIs have been introduced as well as the active enantiomeric form of one, (S)-citalopram. All are structurally distinct from the tricyclic molecules (Figure 30-4). These drugs have fewer adverse effects than the tricyclics and have become very popular. D. MONOAMINE OXIDASE (MAO) INHIBITORS MAO inhibitors may be classified as hydrazides, exemplified by the C-N-N moiety, as is the case with phenelzine and isocarboxazid (no longer marketed); or nonhydrazides, which lack such a moiety, as with tranylcypromine (Figure 30-5). Tranylcypromine closely resembles dextroamphetamine, which is itself a weak inhibitor of MAO. Tranylcypromine retains some of the sympathomimetic characteristics of the amphetamines. The hydrazides appear to combine irreversibly with the enzyme, whereas tranylcypromine has a prolonged duration of effect even though it is not bound irreversibly. These older MAO inhibitors are nonselective inhibitors of both MAO-A and MAO-B. Selegiline, an MAO inhibitor used in Parkinson's disease that is selective for MAO-B at low doses but less selective at higher doses, has been approved for the treatment of major depression
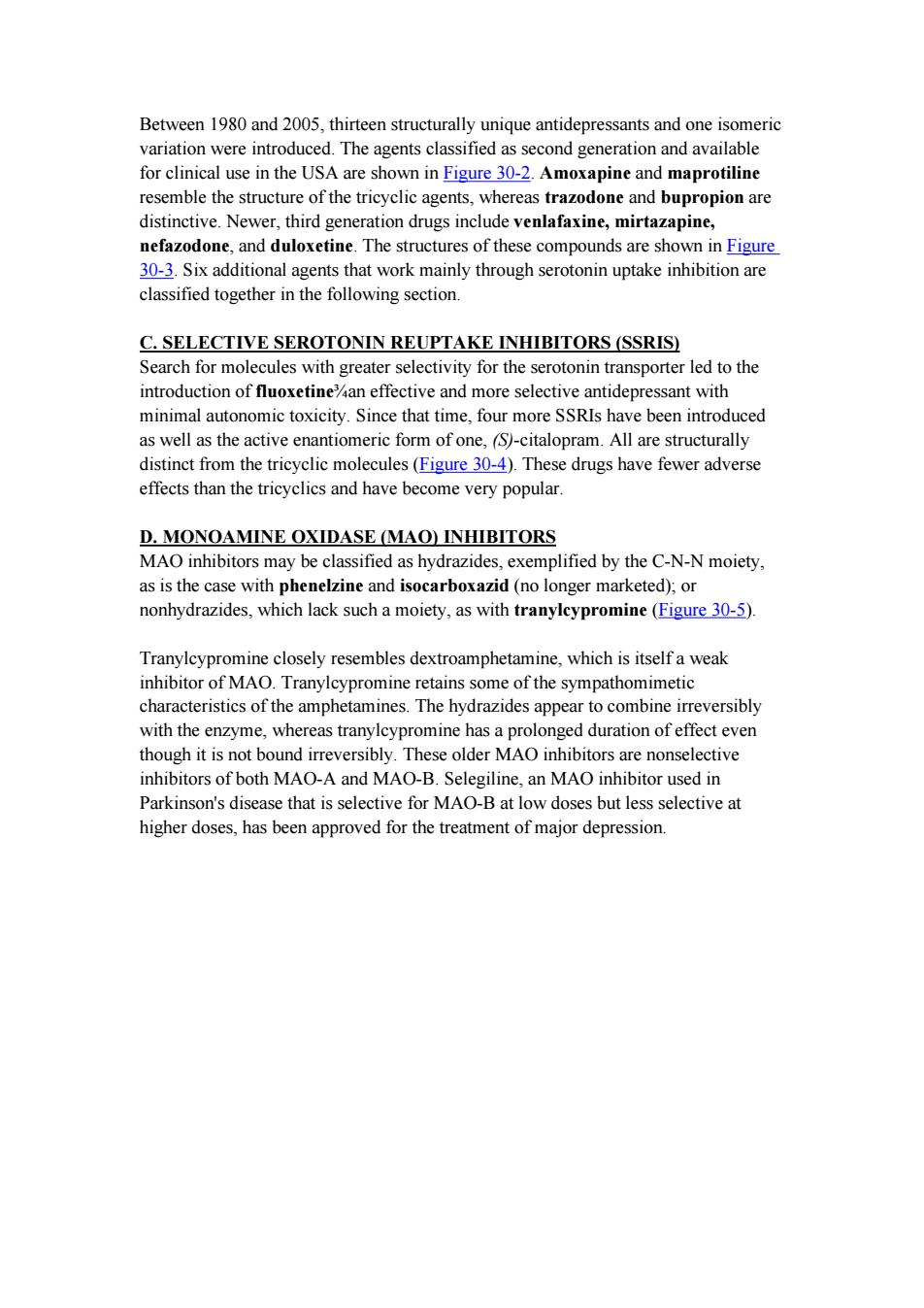
R:-(CH2)N(CH3)2 R:=CH(CH2)2N(CH3h2 R1:=CH(CH2)N(CHab R2:H Imipramine Amitriptyline Doxepin Rj:-(CH2lNHCH3 R:=CH(CH22NHCH3 R2:H Nortriptyline Desipramine R:-(CH2lN(CHgl2 R:-(CH2lgNHCH3 R2:-C Protriptyline Clomipramine R:-CH2CH(CH3)CH2N(CH3)2 R2:H Trimipramine Figure 30-1.Structural relationships between various tricyclic antidepressants (TCAs). NH CH2一CH2一CH2一NH一CH3 Amoxapine Maprotiline 0 CH2-CH2一CH2一 CH -NH一C(CH3)3 CHa Trazodone Bupropion Figure 30-2.Second-generation antidepressants
Figure 30-1. Structural relationships between various tricyclic antidepressants (TCAs). Figure 30-2. Second-generation antidepressants

-N CH3 N CH3 HO CH30 Mirtazapine Venlafaxine CH2CH2 0-CH2一CH2一N CH2一CH2一CH2 0 Nefazodone CH2、 NHCH3 CH CH2 Duloxetine Figure 30-3.Newer(third-generation)antidepressants 0-CH CH2 CH2CH2NHCH3 Fluoxetine Paroxetine NHCH3 Sertraline NC、 F3C CH2CH2CH2CH2OCH3 CH3 CH2CH2CH2N 0-CH2CH2NH2 Fluvoxamine Citalopram Figure 30-4.Selective serotonin reuptake inhibitors(SSRIs)
Figure 30-3. Newer (third-generation) antidepressants. Figure 30-4. Selective serotonin reuptake inhibitors (SSRIs)