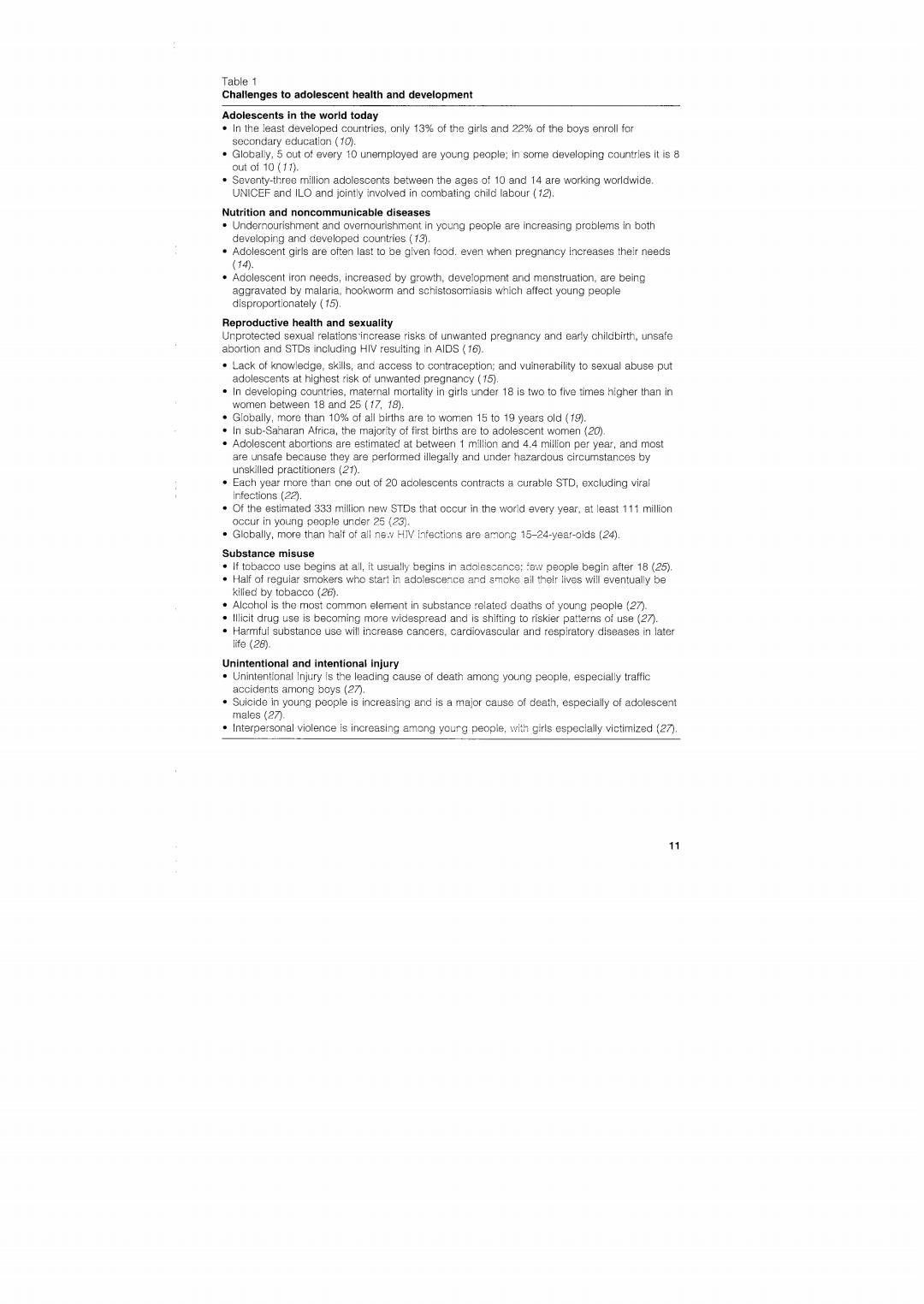
Table 1 Challenges to adolescent health and development Adolescents in the world today In the least developed countries,only 13%of the girls and 22%of the boys enroll for secondary education (10). Globally,5 out of every 10 unemployed are young people;in some developing countries it is 8 out of 10 (11). Seventy-three million adolescents between the ages of 10 and 14 are working worldwide. UNICEF and ILO and jointly involved in combating child labour (12) Nutrition and noncommunicable diseases Undernourishment and overnourishment in young people are increasing problems in both developing and developed countries (73). Adolescent girls are often last to be given food.even when pregnancy increases thelr needs (149 Adolescent iron needs,increased by growth,development and menstruation,are being aggravated by malaria.hookworm and schistoscmiasis which affect young people disproportionately (15) Reproductive health and sexuality Unprotected sexual relations increase risks of unwanted pregnancy and early childbirth,unsafe abortion and STDs including HIV resuiting in AlDS (16). Lack of knowledge,skills,and access to contraception;and vuinerability to sexual abuse put adolescents at highest risk of unwanted pregnancy(15). In developing countries,maternal mortality in girls under 18 is two to five times higher than in women between 18 and 25 (17,18). Globally,more than 10%of all births are to women 15 to 19 years old (19). .In sub-Saharan Africa,the majority of first births are to adolescent women(20) Adolescent abortions are estimated at between 1 million and 4.4 million per year,and most are unsafe because they are performed illegally and under hazardous circumstances by unskilled practitioners (21). Each year more than cne out of 20 adolescents contracts a curable STD,excluding viral infections(2☑. Of the estimated 333 million new STDs that occur in the world every year,at least 111 million occur in young people under 25(23). Globally,more than half of all ne.y HIV infections are among 15-24-year-oids (24) Substance misuse If tobacco use begins at all,it usually begins in adolescence:ow people begin after 18(25) ·Half of reguiar smo ers who stari in adolescence and smoke all their lives will eventually be killed by tobacco (26). Alcohol is the most common element in substance related deaths of young people(27) lllicit drug use is becoming more widespread and is shifting to riskier patterns of use(27). Harmful substance use will increase cancers,cardiovascular and respiratory diseases in later 1fe(280. Unintentional and intentional injury Unintentional injury is the leading cause of death among young people,especially traffic accidents among boys (27). Suicide in young people is increasing and is a major cause of death,especially of adolescent males(2刀 Interpersonal violence is increasing among yourg peopie,with girls especially victimized (27). 11

pregnancy and childbirth).This is discussed in greater detail in section 3.3.Table 2 contains a listing of health problems and un- healthy behaviour that significantly affect public health in the short and long terms.One clear indication of the burden of morbidity and mortality is provided by calculating so-called "disability adjusted life years"(DALYs)-a concept illustrated in Box 1. Certain risk factors for health problems are peculiar to adolescents, although there are risk factors common to both adolescents and adults.For example,adolescents may engage in sexual activity before they are fully aware of the long-term consequences of their actions,the need for protection against STDs or of the avail- ability of reproductive health services. Some health problems may have more serious consequences for adolescents than adults;early childbirth is a case in point.Female adolescents'pelvic bones continue to grow for several years after growth in height has been completed.If pelvic growth is not com- pleted before childbirth,there is an increased chance of obstructed labour and vesicovaginal fistulae. Table 2 A classification of the health problems and health-related behaviour of young people in developing countries,with illustrative examples (25) Diseases Diseases and Diseases which Diseases and Diseases particular to unhealthy manifest unhealthy which affect young people behaviour which themselves behaviour of young people affect young people orimarily in young people less than disproportionately vouna people. whose malor children,but but originate implications are more than in childhood on the young older adults person's future health -Disorders of "Maternal mortality Chagas *STDs (including Malnutrition seconaary morbidity aisease HIV) Malaria sexual *STDs (including *Rheumatic *Leprosy "Gastroenteritis development HIV) heart disease *Dental disease *Acute "Difficulties *Tubercuiosis Polio respiratory with *Schistosomiasis Behaviour: infections psychosocial "Intestinal helminths *Tobacco use development Mental disorders "Poor diet Suboptimal *Lack of adolescent Benaviour: exercise growth spurt "Alcohol abuse *Unsafe sexual *Other substance practices abuse *Injuries NB Young eople account f or a substantial nbe of case because they form a large proportion of the popu

Box 1 Estimates of the burden of disease among young people The"Disability Adjusted Life Year"(DALY)is a measure used to quantify burden:it is a time-based measure which captures the impact of prema- ture death(in years)and time(in years)lived with a disability.One DALY is one lost year of healthy life.A recalculation of the Global Burden of Disease estimates among adolescents,youth and young people(29) gave the following findings: The burden of disease and injury between the ages of 10 and 24 represents 15%of the total burden worldwide. Ninety percent of the DALYs are lost in developing countries. Forty-two percent of DALYs result from noncommunicable diseases, 29%from injuries and 29%from communicable,maternal,perinatal and nutritional conditions. The DALY distribution for adolescents and youths is very different from the pattern observed in children or adults,with STD,HIV and maternal conditions,depression,alcohol and drug use,injuries and road traffic accidents predominating among adolescents. Patterns of burden are very distinct between the sexes:DALY rates for injuries(and for suicide)tend to be twice as high among males as among females. The exception to this are the extreme suicide rates in females in China and India which are higher than those among boys. There are health problems which need to be dealt with differently in adolescents than in adults and children-clearly,the traditional approach to preventing and managing the health problems of adults is not always effective in dealing with those of adolescents. The cyclical and complex ways in which the different levels of causation correlate are illustrated in Figure 2(30).Early education programmes for the prevention of smoking sought to inform about the long-term health problems of smoking.The programmes often used scare tactics,futilely relying on the theory that fear of consequences would deter adolescents from smoking.More suc- cessful programmes now focus on the developmental needs of ado- lescents.They emphasize the short-term physical and social consequences of smoking (such as the disagreeable odour on clothes and on the breath,stains on the fingers and teeth,and reduced exercise and sports performance).In addition,they pre- pare adolescents to resist social and peer pressure by helping them strengthen their skills. Adolescents are neither children nor adults,though they share some of the characteristics of both groups.Furthermore,they are not a 13

Figure 2 Young people's health and development-levels of causation and impact Health and development problems Increased child mortality,low birth weight,increased fertility,heart disease,cancer and other tobacco-related causes of death and disease;poor parenting skills; decreased productivity.unemployment and poverty:chronic disease and disability HIV/AIDS and other sexually transmitted diseases;prostitution,teenage pregnancy, abortion,and maternal death;intentional and unintentional injuries,disabilities,and death:school absenteeism and drop-outs;poor nutrition and common endemic diseases;illiteracy 2 High risk behaviour Substance abuse(including the use of alcohol and tobacco):engaging in unwanted and/or unsafe sex;unhealthy eating habits;situations which increase the likelihood of accidents and violence:negative and possibly harmful peer relationships and affiliations;living on the streets,child involvement in wars,child sexual exploitation harmful work conditions Immediate causes Inadequate information and skills;poor access to education and health services. unsafe and unsupportive environment(from family and friends;service providers: policies/legislation and the media);exploitation and abuse Underlying factors Poverty,rapid social change and urbanization;gender,ethnic and other forms of discrimination;unemployment:social values and norms;war and emergencies homogeneous group;their needs vary with their stages of develop- ment and life circumstances.These facts are not just of academic interest;they have tremendous public health implications. Adolescents tend to view health problems very differently from the adults concerned about their welfare.For instance,although health care providers regard HIV/AIDS as a serious public health problem, adolescents do not always do so (even in parts of the world with high levels of HIV infection and HIV-related illnesses).On the other hand. acne which health care providers may consider trivial is considered a serious problem by adolescents of both sexes (31). Adolescents with health problems do not always turn to health care providers and to health services for help.Depending on the problem and their perception of it,they seek help from various individuals and organizations around them.Their perception of what assistance they 14

can get from these individuals and organizations determines their reaction.A study using the narrative research method in 11 African countries shows,on the basis of young people's accounts concerning pregnancy testing,care or termination,that they did not consult health professionals.When presented with various options,the doctor or health services were the least likely option(32).There is need for concerted efforts to prevent the health problems referred to above, and respond to them if and when they arise.When programming for this,it is essential to be cognizant of the perceptions and tendencies of adolescents,and to tailor preventive and curative approaches to their special needs (see section 4). Concerning the guiding concepts of programming for adolescent health and development.the twin goals set out in this section are interrelated and cannot meaningfully be treated in isolation.To programmatically address the issues of individual development of young people minimizes the emergence of specific health and behavioural problems.Conversely,the existence of specific health problems in the lives of young people will adversely affect their devel- opment,and undermine efforts to develop the competencies and skills they need to realize their full potential.Box 2 summarizes the need for programmes for young people to look beyond problem- reduction and towards broader approaches. Guiding concepts 3.1 Background There are many facets of human development:the physical,emo- tional,intellectual,social,moral,spiritual,and aesthetic aspects.Ado- lescence is a time of very rapid,albeit uneven development.There are differences in the rate and degree to which each aspect of develop- ment takes place within the individual,and these differences exist between young people of the same age and sex,of different sexes,and from different sociocultural backgrounds.Development requires an active mind and body,and social interaction.For development to take place,it is essential that opportunities are provided for behaviour that contributes to it.A loving and supportive family and safe envi- ronment are more likely than not to foster positive adolescent development Adolescent health,like adolescent development,is a positive concept It comprises physical,mental and social well-being and not merely the absence of disease or infirmity (WHO Constitution)and,like devel- opment,it is closely related to adolescent behaviour.However,many