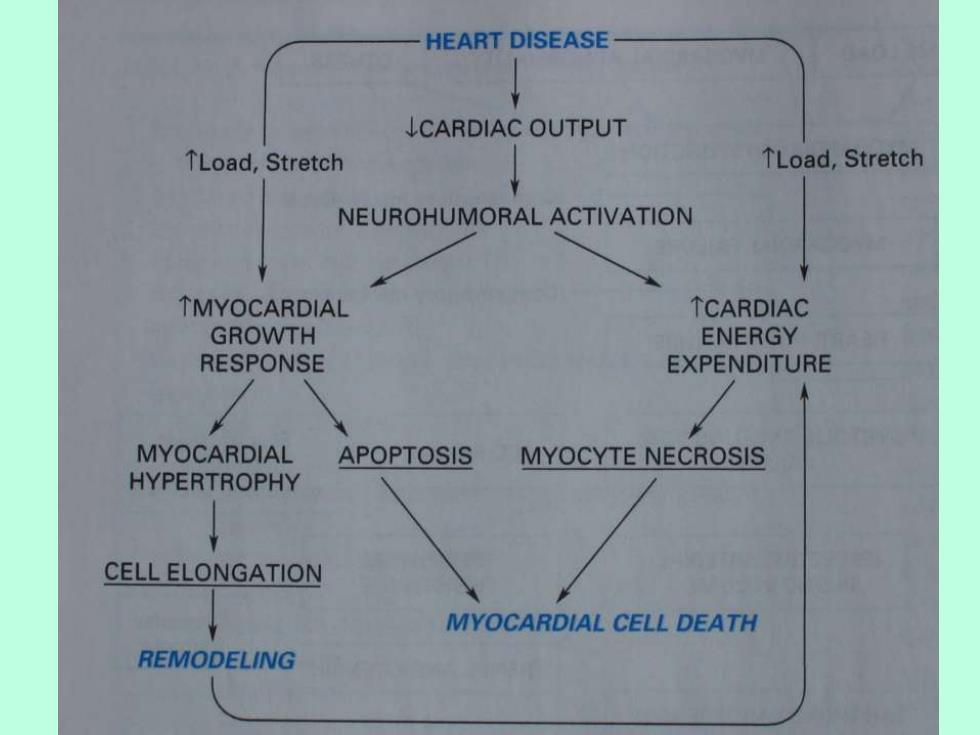
HEART DISEASE LCARDIAC OUTPUT TLoad,Stretch TLoad,Stretch NEUROHUMORAL ACTIVATION TMYOCARDIAL TCARDIAC GROWTH ENERGY RESPONSE EXPENDITURE MYOCARDIAL APOPTOSIS MYOCYTE NECROSIS HYPERTROPHY CELL ELONGATION MYOCARDIAL CELL DEATH REMODELING
VENTRICULAR REMODELING (HYPERTROPHY AND DILATATION) When one portion of ventricle is disabled, an increase of ventricular volume slowly occurs.This involves increased myocyte length,with the limit being at the level of the sarcomere at 2.2um.With systolic overload,compensatory hypertrophy occurs with the addition of sarcomeres in parallel,leading to a lateral thickening of the myocyte while sarcomere length does not change. 17
17 VENTRICULAR REMODELING (HYPERTROPHY AND DILATATION) When one portion of ventricle is disabled, an increase of ventricular volume slowly occurs. This involves increased myocyte length, with the limit being at the level of the sarcomere at 2.2um. With systolic overload, compensatory hypertrophy occurs with the addition of sarcomeres in parallel, leading to a lateral thickening of the myocyte while sarcomere length does not change
Acute dilatation is also limited by the sarcomere, which at 2.2 um attains maximum force.Beyond this point,stiffness of the sarcomere occurs and the myocardium becomes very large and resting tension rises to high levels.When distending forces become chronic,the addition of new sarcomeres occurs in series.Dilatation of the ventricle also adds to the load.Tension in the wall rises with increased volume at the same pressure.This results in some lateral growth of myocytes,although elongation is the major alteration
Acute dilatation is also limited by the sarcomere, which at 2.2 um attains maximum force. Beyond this point, stiffness of the sarcomere occurs and the myocardium becomes very large and resting tension rises to high levels. When distending forces become chronic, the addition of new sarcomeres occurs in series. Dilatation of the ventricle also adds to the load. Tension in the wall rises with increased volume at the same pressure. This results in some lateral growth of myocytes, although elongation is the major alteration
In addition,fuctional mitral regurgitation may result from excessive ventricular volume,and this adds to the volume overload.When increased systolic tension occurs,myocyte hypertrophy due to the laying down of sarcomeres in parallel is accomplished by biochemical alterations in both the contractile proteins and activating membrane systems.The regulation of sarcomere assembly is not well understood,but clearly mechanical forces must be sensed that,in turn,alter gene transcription via complex stretch-activated pathways
In addition, fuctional mitral regurgitation may result from excessive ventricular volume, and this adds to the volume overload. When increased systolic tension occurs, myocyte hypertrophy due to the laying down of sarcomeres in parallel is accomplished by biochemical alterations in both the contractile proteins and activating membrane systems. The regulation of sarcomere assembly is not well understood, but clearly mechanical forces must be sensed that, in turn, alter gene transcription via complex stretch-activated pathways
In addition to the synthesis of sarcomeres in series with preexisting sarcomeres,"slippage"of myofibrils and myocardial fibers and rearrangement of myocardial fibers may occur. Excessive stretch of myocytes can lead to myocyte death,which may lead to further heart failure. Nonuniformity of myocardial contraction and functional mitral regurgitation also contribute to heart failure.The discoordinated contraction is particularly troublesome for patients with underlying cardiac dysfunction
In addition to the synthesis of sarcomeres in series with preexisting sarcomeres, “slippage” of myofibrils and myocardial fibers and rearrangement of myocardial fibers may occur. Excessive stretch of myocytes can lead to myocyte death, which may lead to further heart failure. Nonuniformity of myocardial contraction and functional mitral regurgitation also contribute to heart failure. The discoordinated contraction is particularly troublesome for patients with underlying cardiac dysfunction